This article may be too technical for most readers to understand. (August 2016) |
An accessory auricle is a congenital anomaly typically seen as a skin coloured nodule, most frequently just to the front of the ear.[1][2]
| Accessory auricle | |
|---|---|
 | |
| Specialty | Dermatology |
Signs and symptoms
edit
The general presentation is of a skin-covered nodule, papule, or nodule of the skin surface, usually immediately anterior to the auricle.[2] However, it may be anywhere within the periauricular tissues.[2] Bilateral presentation can be seen.[2]
Genetics
editA study of a family with 11 affected showed the accessory auricle were inherited in an autosomal dominant manner.[3]
Diagnosis
edit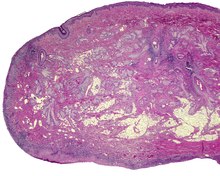
The lesions presents as a nodule or papule, either sessile or pedunculated. They may be soft or have a cartilaginous structure. By histologic examination, it is a recapitulation of normal external auricle. There will be skin, cartilaginous structures, and cartilage (although the last is not seen in all variants of this disorder).[4][5] Some investigators believe that the tragus is the only hillock which is derived from the first branchial arch. This is clearly suggestive that true cases of accessory auricle represent a true duplication of the hillocks that were part of the second branchial arch.[6] The second ear appears as a mirror image folded forward and lying on the posterior cheek.[citation needed]
Differential diagnosis
editThese structures are distinctly different from squamous papilloma and benign teratoma.[citation needed]
Classification
editThe several components or degrees of development range from an ear tag, preauricular appendage, preauricular tag, or accessory tragus, to supernumerary ears or polyotia.[7] It is a relatively common congenital anomaly of the first branchial arch or second branchial arches. Other anomalies may be present concurrently, including cleft palate, cleft lip, or mandibular hypoplasia. There is a known association with Goldenhar syndrome (oculo-auriculo-vertebral syndrome)[8] and with Wildervanck syndrome.[9][10][11] There may also be an association with congenital cartilaginous rest of the neck.[citation needed]
Management
editSimple surgical excision is curative.[12] The recommended treatment is that the skin is peeled off the extra-auricular tissue and protruding cartilage remnants are trimmed.[13] Normal appearance is achieved in majority of cases. The reconstruction successful in true cases of accessory auricle, as it also is in individuals with auricular appendages.[14][15]
Epidemiology
editThese lesions usually present in neonates, although they may not come to clinical attention until adulthood (for cosmetic reasons). There is no gender predilection. They are present in approximately 3–6 per 1000 live births.[16]
References
edit- ^ Hwang, Jungil; Cho, Jaeyoung; Burm, Jin Sik (September 2018). "Accessory auricle: Classification according to location, protrusion pattern and body shape". Archives of Plastic Surgery. 45 (5): 411–417. doi:10.5999/aps.2018.00430. PMC 6177632. PMID 30282411.
- ^ a b c d Cardesa, Antonio (2016). "8. Ear and temporal bone". In Franchi, Alessandro; Slootweg, Pieter J.; Gale, Nina; Ann, Sandison (eds.). Pathology of the Head and Neck. Springer. p. 397. ISBN 978-3-662-49670-1.
- ^ Yang, Y; et al. (2006). "A locus for autosomal dominant accessory auricular anomaly maps to 14q11.2–q12". Human Genetics. 120 (1): 144–147. doi:10.1007/s00439-006-0206-1. PMID 16775710. S2CID 1196716.
- ^ Jansen, T.; Romiti, R.; Altmeyer, P. (2000). "Accessory tragus: Report of two cases and review of the literature". Pediatric Dermatology. 17 (5): 391–394. doi:10.1046/j.1525-1470.2000.017005391.x. PMID 11085670. S2CID 19325370.
- ^ Brownstein, M. H.; Wanger, N.; Helwig, E. B. (1971). "Accessory tragi". Archives of Dermatology. 104 (6): 625–631. doi:10.1001/archderm.1971.04000240049006. PMID 5131708.
- ^ Stevenson, Roger E.; Hall, Judith G. (2005). Human Malformations and Related Anomalies (2nd ed.). Oxford University Press. pp. 339–340. ISBN 978-0199748082.
- ^ Lam, J.; Dohil, M. (2007). "Multiple Accessory Tragi and Hemifacial Microsomia". Pediatric Dermatology. 24 (6): 657–658. doi:10.1111/j.1525-1470.2007.00560.x. PMID 18035991. S2CID 19272462.
- ^ Konaş, E.; Canter, H. I.; Mavili, M. E. (2006). "Goldenhar complex with atypical associated anomalies: Is the spectrum still widening?". Journal of Craniofacial Surgery. 17 (4): 669–672. doi:10.1097/00001665-200607000-00011. PMID 16877912.
- ^ Tadini, G.; Cambiaghi, S.; Scarabelli, G.; Brusasco, A.; Vigo, P. (1993). "Familial occurrence of isolated accessory tragi". Pediatric Dermatology. 10 (1): 26–28. doi:10.1111/j.1525-1470.1993.tb00006.x. PMID 8493161. S2CID 20872067.
- ^ Gao, J. Z.; Chen, Y. M.; Gao, Y. P. (1990). "A survey of accessory auricle anomaly. Pedigree analysis of seven cases". Archives of Otolaryngology–Head & Neck Surgery. 116 (10): 1194–1196. doi:10.1001/archotol.1990.01870100088019. PMID 2206506.
- ^ Resnick, K. I.; Soltani, K.; Bernstein, J. E.; Fathizadeh, A. (1981). "Accessory tragi and associated syndromes involving the first branchial arch". The Journal of Dermatologic Surgery and Oncology. 7 (1): 39–41. doi:10.1111/j.1524-4725.1981.tb00591.x. PMID 7204730.
- ^ Pan, B.; Qie, S.; Zhao, Y.; Tang, X.; Lin, L.; Yang, Q.; Zhuang, H.; Jiang, H. (2010). "Surgical management of polyotia". Journal of Plastic, Reconstructive & Aesthetic Surgery. 63 (8): 1283–1288. doi:10.1016/j.bjps.2009.06.037. PMID 19617017.
- ^ Scott-Brown's Otorhinolaryngology (7th ed.). Hodder Arnold. 2016-06-15. p. 969. ISBN 978-0-340-808-931.
- ^ Ku, PK; Tong, MC; Yue, V (1998). "Polyotia- a rare external ear anomaly". International Journal of Pediatric Otorhinolaryngology. 46 (1–2): 117–20. doi:10.1016/S0165-5876(98)00152-9. PMID 10190712.
- ^ Bendor-Samuel, RL; Tung, TC; Chen, YR (1995). "Polyotia". Annals of Plastic Surgery. 34 (6): 650–2. doi:10.1097/00000637-199506000-00015. PMID 7661545. S2CID 220587660.
- ^ Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. p. 894. ISBN 978-1-4160-2999-1.
Further reading
edit- Lester D. R. Thompson; Bruce M. Wenig (2011). Diagnostic Pathology: Head and Neck. Hagerstown, MD: Lippincott Williams & Wilkins. pp. 7:2–3. ISBN 978-1-931884-61-7.