Talk:Ketamine/Archive 1
| This is an archive of past discussions about Ketamine. Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |
| Archive 1 | Archive 2 | Archive 3 |
Synthesis
Synthesis of ketamine can start with the reaction of cyclopentyl magnesium bromide (cyclopentyl grignard) and o-chlorobenzonitrile. After hydrolysation, a ketone is formed: o-chlorophenyl-cyclopentyl ketone.
This is followed by alpha bromination of the ketone, which gives alpha-bromo (o-chlorophenyl)-cyclopentyl ketone. Dissolving this ketone in methylamine leads to 1-hydroxycyclopentyl-(o-chlorophenyl)-ketone-N-methylimine.
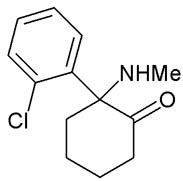
Heating of this alpha-hydroxy-imine leads to a rearangement (cyclopentyl to cyclohexyl) and gives the final product 2-Methylamino-2-(o-chlorophenyl)-cyclohexanone, known as ketamine. --UgPanda 22:42, 26 May 2006 (UTC)
Remission lasted no more than seven days
This article says "More than a third continued to report such a benefit after seven days, and nearly a third reported a complete end of symptoms" (emphasis mine). Is there a source on the statement "Remission lasted no more than seven days"? --π! 15:33, 8 August 2006 (UTC)
- JAMA Psych Archives says subjects were tested (infused) on 2 days, a week apart; they were rated at several intervals, up to 7 days "postinfusion". "Thirty-five percent of subjects maintained response for at least 1 week." No conclusions can be drawn about greater than a week. It also states "71% met response and 29% met remission criteria the day following"; I wonder if the 29% is the "nearly a third reported complete end of symptoms" mentioned in the Post article. I notice that 71% + 29% = 100%, so I wonder what "remission" means. Unfortunately, I don't have access to the actual full text of the report.
Emergence Phenomena and Side Effects
There's a great article at emedicine.com about the advantages of ketamine as an anesthetic and analgesic, particularly in emergency situations. The risk of emergence phenomena, and their severity, in clinical practice, have been blown out of proportion in the developed world. They can be abolished almost completely simply by the preadministration of a benzodiazepine or one of a couple of other types of drugs. In the case that someone does have an emergence reaction, simple reassurance is enough to get them through it. It's still used widely in the developing world as a surgical anesthetic because its safety profile is so superior to other anesthetics and it doesn't require the same kind of expensive infrastructure that traditional anesthesia methods do, or an anesthesiologist. Its utility as a clinical drug has been neglected in the article and its hallucinatory side effects played up. I've got nothing against k-space, but there's a big difference between using the stuff in the pursuit of out-of-body phenomena and the like, and using it to do surgery or change burn dressings. Put simply, in a medical setting there is no excuse for anyone to have a negative recovery from ketamine. I'll be editing the article to reflect its clinical use as I have the opportunity. Porkchopmcmoose 18:24, 31 August 2006 (UTC)
Fix the Image?
"Stereochemistry shown in the picture is INCORRECT. The correct is opposite one." Anyone want to fix this up? It's at the bottom of the "recreational use" section. Hanzolot 00:08, 7 September 2006 (UTC)
- —Fixed. Porkchopmcmoose 19:23, 10 September 2006 (UTC)
- I didn't just mean remove the sentence, like, is the actual stereochemistry incorrect? As in, should the picture be changed? Hanzolot 23:11, 10 September 2006 (UTC)
- I did change the picture of the ketamine enantiomers to one I made showing the proper stereochemistry. The previous version(s) had it flipped. Or are you referring to something else? Porkchopmcmoose 00:35, 3 October 2006 (UTC)
- I didn't just mean remove the sentence, like, is the actual stereochemistry incorrect? As in, should the picture be changed? Hanzolot 23:11, 10 September 2006 (UTC)
Structure
What is the correct structure of ketamine? There are two different structures on this page:
 and File:Ketaminpics.gif
and File:Ketaminpics.gif
{kind=link}
At ketamine.com they have yet another structure, which is the same as was once on this page: http://www.ketamine.com/ketamine-structure.jpg
{kind=link}
This page has the same as on ketamine.com, so do this page and this page. Unless someone can proof this is wrong, I'm changing it tomorrow. -- Sander 18:00, 2 January 2006 (UTC)
- Those last two structures are incorrect. Ketamine is an amine, and those last two structures (the ones with the chair cyclohexane conformation) completely omit ketamine's methylamino group. I hadn't noticed that before; they should be fixed or removed from the article. The structure you linked to (http://www.ketamine.com/ketamine-structure.jpg) is exactly equivalent to the first structure (Image:Ketamine.png), the orientation is just rotated and the rings flipped.
- Please do not remove the drugbox image, however I will fix the enantiomer image if no one else gets around to it over the next few days. --Bk0 (Talk) 00:14, 3 January 2006 (UTC)
- I'm really blind... You're right, they are the same. So just the other image needs fixing. Thanks for correcting me :) -- Sander 12:19, 3 January 2006 (UTC)
Hi, I made a picture of the S(+) enantiomer. I based the structure on one of my textbooks. As far as I could tell, it seems correct.
.png){kind=link}
Conflicting information on analgesic use
There seems to be two statements in the 'Medical Use' section that contradict each other:
Ketamine is a co-analgesic, requiring a concomitant low-dose opioid to be effective.
Ketamine is also a potent analgesic and can be used in sub-anaesthetic doses to relieve acute pain.
One of these really should go. Even if somehow both are true, they should be combined into a single statement.
- Pacula 11:11, 20 October 2005 (UTC)
I agree it's confusing. I believe the first reference is to chronic pain; the ketamine inhibits the pain due to wind-up or central sensitization, but an opiod is often still needed by chronic pain patients for muscle pain, etc that does not originate from the nervous system.
In acute pain however, a low dose of ketamine is usually sufficient to relieve whatever the source of pain may be.
It seems as though the two could be discussed in the same paragraph at least to make things more clear.
Nervis Breakdown 06:13, 5 November 2005 (UTC)
http://www.emedicine.com/emerg/topic802.htm
Pain is a complicated system involving many factors. Ketamine has analgesic properties in its own right, although as with many other analgesics the effect may be synergistic (increased) if analgesics with different mechanisms of action are used together - think paracetamol & codeine. The limitation of ketamine as a pure analgesic is its psychotropic effect, which dominates at doses close to that requires for analgesia. —The preceding unsigned comment was added by Iceinthecider (talk • contribs) .
- Do you have any references for the analgesic properties of ketamine? I have always heard that ketamine is effective only when combined with an opioid (the analgesia of the combination is greater than either alone) but ketamine by itself is not considered an effective analgesic. --Bk0 (Talk) 16:12, 8 October 2006 (UTC)
The conflicting statements may be a result of another effect of Ketamine. It's also used as a local (typically topical) anesthetic, which is thought to be caused by a totally different mechanism (blocking sodium channels) than the mechanism that causes the more widely known effects. You can read about this in this well referenced article: http://www.anesthesia-analgesia.org/cgi/content/full/96/4/1019#R4-122335
I've already modified the article to indicate the local anesthetic use, and suspected mechanism of action. --Vellmont 01:26, 13 December 2006 (UTC)
Schedule II or III
This change was made with no discussion. Does anyone know which is the correct schedule for this drug? Is this sneaky vandalism? Thanks, delldot | talk 05:39, 22 December 2006 (UTC)
- After a quick google search, it looks to me like it's schedule III. So I've reverted and added a reference. If you have more info, go ahead and make the necessary changes or discuss them here. Peace, delldot | talk 05:52, 22 December 2006 (UTC)
Ketamine
I'm a NOOB, but according to the government of Canada website that I checked (I had supplied a link) Ketamine is a Schedule I drug here in Canada.
PS I was the one that edited... —The preceding unsigned comment was added by Suitsme (talk • contribs) 13:09, 22 December 2006 (UTC).
We need more citations
This ketamine article needs way more citations, despite the many that I've put in. We especially need them in the Neuropharmacology and Recreational Use sections, since they're the most important sections and should be referenced. I'm no expert on this stuff, and the neuropharmacology section has some very advanced information, so whoever wrote that should definitely cite their sources. For the recreational use section, I feel that erowid citations would be acceptable, so go right ahead. Jolb 22:13, 23 February 2007 (UTC)
out of body experience..... exaggerated?
The drug was first given to American soldiers during the Vietnam War, but today in the developed world its use on humans has been dramatically curtailed because of exaggerated concern about its potential to cause emergence phenomena including out-of-body experiences in clinical practice.
I don't know much about the drug, which is what led me here, but after reading this paragraph, it seemed the use of exaggerated is very biased and not encyclopedic, although i did not remove it as i have not and do not plan on looking at the source cited in the paragraph. Kmccusker2 06:03, 12 March 2007 (UTC)
- Agreed, let me change it. Jolb 06:07, 12 March 2007 (UTC)
well, ok, that was a quick response, in the time it took me to click the link for the reference out of curiosity (nothing on exaggeration in source) you had already responded. impressive. Kmccusker2 06:16, 12 March 2007 (UTC)
- Lol, I keep a close eye on the few articles in my watchlist. Jolb 06:19, 12 March 2007 (UTC)
An epistemological problem
If a large enough amount is taken the user may go into or through a "K-hole", a state of wildly dissociated experience in which other worlds or dimensions that are difficult to describe with language are said to be perceived, all the while being completely unaware of one's individual identity or the outside world. . . . Users often do not remember this part of the experience after regaining consciousness.
How could this possibly be known? Obviously no one else knows anything about someone's subjective experience but what he reports, so if he can't remember it, where's the information come from? --Ian Maxwell 18:12, 2005 August 25 (UTC)
- Well, it says "often", presuming that some people remember their trip down the keyhole and emerged with some recollections. But it is baloney and should be removed. JFW | T@lk 20:22, 25 August 2005 (UTC)
- The "often do not remember" comment probably should be modified... the way it can work with some people is that they will experience several K-holes before they remember one or the earlier ones, though in my experience this is not common. Similar to dreaming: a person can forget their dreams, though we know that basically everyone dreams when sleeping, and the forgetter will at times recall a past dream or be able to remember a new one. —Tarnas 02:23, 26 August 2005 (UTC)
- Yes i think this is poorly put. Is it refering to a state of complete unconciousness, or an extreme disassociated state. It is possible to go into a K-hole (whatever that is, and its slightly different from all people) while being in an awake state and semi aware of situational factors (though these are often distorted as part of the trip).
- Officially modified! —Tarnas 03:43, 26 August 2005 (UTC)
Like it says, it's an extremely dissociated state. From how it was described in real life by a friend, the K-Hole is when you're on Ketamine to the point that you lose all touch with reality. 4.234.51.29 21:54, 25 January 2007 (UTC)
Although I see the problem with the logic of the sentence it can make sense. For example (hypothetically), if I when going into the hole I was in one room and when coming out of it I found myself in another room wearing wet clothes yet had no recollection of making the transition then I could state with certainty that I did not remember what happened although I know something must have. Speedything 13:42, 25 April 2007 (UTC)
Opioid
this change claims that K is an opioid, however I cant (quickly) see any source for this and a search indicates the old text was correct[1]. John Vandenberg 11:09, 20 June 2007 (UTC)
Recent finding on damage from abusing the Street stuff
On 21 June 2007 Hong Kong Medical Journal has put up a report regarding to the abuse of "Street" K, with the title as Street ketamine'–associated bladder dysfunction: a report of 10 cases. (Click the link to get there). The report has shown that the long term abuse of the K has caused damage to the liver, gall bladder and even a case of acute renal failure, though the scientist are speculating if this is caused by other toxins or chemical reactions. I was wondering if that this finding (along with source) can be included into the article as well. Can anyone answer this please? --Blackhawk charlie2003 03:28, 22 June 2007 (UTC)
Repeated Vandalization of References
The extensive reference section of this article has been repeatedly deleted by a vandal. It seems likely that some unscrupulous individual is dedicated to this vandalism, and often does it without numerous subsequent well-intentioned editors noticing, leaving countless readers at a loss to verify the carefully referenced claims in this article. After this vandalism is reverted, the vandal apparently takes his or her time before re-vandalizing this article, probably hoping that it will again go unnoticed for a maximal amount of time.
Is there some kind of mechanism that can be activated to make note of this dedicated vandalism effort that might thereby thwart it? 207.69.140.25 05:09, 27 June 2007 (UTC)
ketamine as a model of schizophrenia
hi, i'm kinda new to wiki, but have added a small paragraph to the "medical use" section regarding k's use as a model of schizophrenia. haven't cited any references, i'll dig them up in a few days. please don't pull it down in the mean time, it's all accurate. 12:00, 28 June 2007 (UTC)
Veterinary use
Is ketamine used by vets worldwide or is illegal in some places? Portillo 09:57, 3 August 2007 (UTC)
I believe it is illegal in Russia - and sadly, so are most other veterianary anaesthetics. Dlh-stablelights 16:49, 15 June 2007 (UTC)
- In the US, ketamine/diazepam and Telazol are the most common anesthetic induction agents. There is significant overlap with human medicine however, so drugs such as propofol and sevoflurane are also used. I imagine it is similar in other industrialized countries however I don't have any direct knowledge outside of the US. --Bk0 (Talk) 00:33, 4 August 2007 (UTC)
Neurotoxicity
In the introduction, it is stated: "Ketamine has a wide range of effects in humans, including analgesia, anesthesia, hallucinations, neurotoxicity, arterial hypertension, and bronchodilation." It stands to reason that neurotoxicty does not have its place in this sentence, even if it is neurotoxic - it just doesn't go with the other adjectives in the sentence. Furthermore, if it used in analgesia and anesthesia, surely its neurotoxic potential is very low -- since there are many other drugs that have such effects, and ketamine would not be used should any actual chances of any kind of toxicity be real. -- Dragonfly31 —Preceding unsigned comment added by 82.10.111.212 (talk) 00:00, 12 December 2007 (UTC)
Neurotoxicity
As far as I know, whether ketamine causes this effect (neurotoxicity) is still a subject of significant debate, and this uncertainty makes it even less appropriate that it should not be listed as a possible effect without a reference. Reb42 (talk) 19:03, 2 January 2008 (UTC)
Adding one more thing - that is not to say that neurotoxicity hasn't ever been observed - just not in humans. Reb42 (talk) 19:09, 2 January 2008 (UTC)
What a mess
Is it just me or does it seem like this article has become a hodgepodge of quotes cut and pasted from various studies? It seems like the conclusions could just be summarized and put into a better structured article. Any objections to a rewrite? --Selket Talk 16:27, 14 August 2007 (UTC)
- It needs a rewrite, some of the stuff is in first person even! Writing in first person is not encyclopedic. I think the first person stuff must have been copied and pasted from some book or interview instead of actually written specifically for this article. 68.2.35.62 06:48, 12 November 2007 (UTC)
agreed! I found "I" statements and realized this page really needed work...or at least for people to stop using the first person and follow wiki guidelines.--75.36.147.93 (talk) 08:37, 24 January 2008 (UTC)
Common Names
Commendable that you guys are urging all the so-called common names listed be added with-source, but just what is so special about the ones already there that they do not need sources? Ketaset and Ketalar, while used in the medical profession, are not exactly the names you hear on street corners. Furthermore, by far the most common name I've heard for ket is horse, far more than "kitty". I'll happily find a source for the horse, but shouldn't the other stuff be removed if there's no source for it? Like "placing a BET"? Jdcooper 03:40, 24 August 2007 (UTC)
Properties in perscribed form My friend was getting a surgery when she thinks she was given this drug, it helped her with her Social Anxiety, she wants to know what exactly she took that day, it was in liquid form, red possibly cherry flavored. —Preceding unsigned comment added by 76.103.48.146 (talk) 17:14, 31 August 2007 (UTC)
What is with the artificial claims and categorizations?
--> "Like the other dissociative anaesthetics DXM and PCP, hallucinations caused by ketamine are fundamentally different from those caused by tryptamines and phenethylamines." /// Oh really? I would fundamentally disagree with this claim and say that the hallucinations are fundamentally similar, though they are different. Though why don't we go through them point by point? And since when did tryptamines and phenethylamines become mutually exclusive classes of substances?
---> "At low doses, hallucinations are only seen when one is in a dark room with one's eyes closed, while at medium to high doses the effects are far more intense and obvious." /// That sounds exactly like how LSD, psilocin bearing mushrooms and other typical hallucinogens works. At lower doses, you only get visuals in low light, but at higher doses, they're obvious in full light.
---> "These effects include changes in the perception of distances, relative scale, colour and durations/time, as well as a slowing of the visual system's ability to update what the user is seeing." /// And certainly nobody ever reports anything similar to that with LSD or mushrooms or mescaline? Changes in perception of distance or size? No, never. Colour? No. Colours don't seem altered while on other hallucinogens. Change in perception of time while on ketamine too? How completely different than with LSD or psilocin? And what's this about inability to update what the user is seeing? You mean that people see trails while on ketamine but that they have a different character than other drugs produce?
---> "Speech often sounds unintelligible i.e. alogia, and auditory hallucinations may occur." // Once again, that sounds absolutely nothing like a high dose LSD experience. Auditory hallucinations?
---> "Colors can also turn to sound and sound into color." // Nobody has ever reported synesthesia with LSD.
What is this absurd desire to separate dissociatives from "phenethylamines" and "tryptamines"? First of all, LSD is BOTH a phenethylamine and tryptamine. Secondly, DXM is both a dissociative and phenethylamine. Heroin is a phenethylamine. While I would agree that dissociatives produce hallucinogenic effects that are different in "character" or "flavour" than 'classic' hallucinogens, to say that they are "fundamentally different" is totally misleading. —Preceding unsigned comment added by 216.99.60.116 (talk) 07:03, 3 March 2008 (UTC)
List of common names
Note the following list has been copied from the delete copy in the article removed by User:Fram with the following edit summary "Removed all references to Nationmaster Encyclopedia: this is an old copy of Wikipedia.)"
The list was moved here to make it easier to restore it when proper references can be obtained
- Cat Tranquilizer [1]
- Horse Tranquilizer [1]
- K[1][2]
- K-Hole[1]
- Keezy [1]
- Kenny [1]
- Ket [1]
- Ketanest [2]
- Ketaset [2]
- Ketalar [2]
- Kez [1]
- Kit-Kat [1]
- Kitties [2]
- Kitty [1]
- Kustard [1]
- Regretamine [1]
- Special K[1]
- Super K [1][2]
- Triple K (KKK) [1]
- Vetamine [1]
- Vitamin K [1][2]
- K wire [1]
- KFC [1]
- Wonky [1]
- ^ a b c d e f g h i j k l m n o p q r s t [http://www.nationmaster.com/encyclopedia/List-of-street-names-of-drugs%23Ketamine#Ketamine List of street names of Ketamine - www.nationmaster.com retreived 11-22-08]
- ^ a b c d e f g [http://www.nationmaster.com/encyclopedia/Ketamine Common names for Ketamine - www.nationmaster.com retreived 11-22-08]
Posted by Dbiel (Talk) 17:14, 3 December 2008 (UTC)
Hey, WTF?
"Ketamine sold illicitly comes from diverted legitimate supplies and semi-legitimate suppliers, or theft, primarily from veterinary clinics. Ketamine is illegaly synthesized in Canada and smuggled into America and sold on the streets. Chinese authorities tried to regulate the production and sale of ketamine more as well in recent years, and several large quantities of ketamine meant for illicit sale were seized by authorities. In the US near its border with Mexico, the drug is most commonly acquired in Mexico, where it can be bought over the counter in veterinary clinics, and smuggled across the border."
Citations, anyone? I'm sure Canadians and Mexicans don't appreciate the accusations here, can someone get some facts or delete this? Thanks. —Preceding unsigned comment added by 99.250.97.108 (talk) 16:00, 27 July 2009 (UTC)
Size of 2D-formulae
Please adjust (enlarge) the size of the 2D-formulae. Thanks --Jü (talk) 19:11, 10 June 2009 (UTC)
- How's that? ⊃°HotCROCODILE...... (talk) 19:27, 10 June 2009 (UTC)
- Looks nice, thanks. --Jü (talk) 19:45, 2 September 2009 (UTC)
Photograph of syringe
The caption reads, "A 30 gauge syringe filled with Ketamine HCL."
The photo is actually a 30 ml syringe with a 20-gauge needle, filled with an unidentifiable clear liquid. The photo seems to serve no purpose whatever, except to show that the photographer happens to have a syringe.
If no one can suggest a good reason why the photo should remain, I'm planning on deleting it. Snezzy (talk) 13:55, 15 September 2009 (UTC)
- It's gone. Snezzy (talk) 13:00, 16 September 2009 (UTC)
Recall
Teva Animal Health ([2]) has issued a voluntary recall of Ketamine Hydrochloride Injection, USP CIII 100mg/mL in 10mL vials for all lot numbers within their expiration dates to the Veterinary Level.
They have nothing on their web page about it, but the FDA has posted the recall information [3]. Should this be included in the main page?
Also, the drug is now a generic, and no longer made only by Pfizer. Acter (talk) 10:28, 28 December 2009 (UTC)Acter
still a mess
- One thing that very much still requires revision is the redundant nature of at least some of the article. Its tone and pace is not very flowing and just not a good read, and of course it rehashes the same information again and again, sometimes with the same citations! I was hoping to get alot out of this article and it can still be saved. Someone flag it, but for what? Cleanup? copy-edit? Someone take the initiative!
-Alan 24.184.184.177 (talk) 03:04, 5 August 2008 (UTC)
No kidding. How about, in the very first sentence, telling the reader WHAT it is used FOR? "It is used in human and veterinary medicine..."? As what? Unless your goal is not to inform. I have to work, so don't have time to read this and do it myself. —Preceding unsigned comment added by 147.80.233.219 (talk) 14:22, 9 June 2010 (UTC)
DXM connection?
I'm not sure having external links to DXM makes sense for this article. Anyone feel a need to leave it in? Overand 05:01, 10 July 2005 (UTC)
- External links don't make sense, though the article references do. --Tarnas 07:20, 1 August 2005 (UTC)
Yeah someone should objectively verify whether the phenomenology is similar to DXM. Oh wait. You can't.
- Along with PCP, DXM/DXO and Ketamine are the three most popularly used/abused dissociative anesthetics of the NMDAR antagonist type. Makes sense enough for me to see a correlation (for an internal link, I need to know what exactly external link you are referencing here it would help if you cited it. Context is what makes sense of things. This extends to this discussion page entry of yours.) Nagelfar (talk) 09:22, 4 August 2010 (UTC)
Medical use: Experimental antidepressant
I added a para about a new (reported today, 7-25-07) study on how ketamine works chemically. I noticed that the footnotes in the "Experimental antidepressant" section are not done properly. They are simple text, and don't have ref tags, so they aren't numbered automatically. Somebody with more time than I have should fix that.
Karlchwe 17:19, 25 July 2007 (UTC)
- Fixed this yesterday. An anon IP butchered the references with a series of cutting and pasting operations that replaced all tags with numbers. [4] They also added a lot of material & references; I tried to fix this carefully rather than revert/remove it, which took a fair amount of work. Madeleine ✉ ✍ 13:35, 3 August 2007 (UTC)
Hey, on the topic there has been another study that appears to have discovered the mechanism of action for ketamine's anti-depressant action. It involves the encouraging of neurons to build stronger and new synapses connecting them in the pre-frontal cortex, the area of the brain that shrinks in depressed people. http://www.medicalnewstoday.com/articles/198483.php —Preceding unsigned comment added by 220.244.54.115 (talk) 07:55, 22 August 2010 (UTC)
cutting with K
When coke is cut with ketamine it gets really damned sticky in your nose. I can't, of course, mention this, as it is original research. I will, however, continue researching. —The preceding unsigned comment was added by 66.124.231.38 (talk) 03:03, 4 April 2007 (UTC).
I assume this would have something to do with how water soluble they are? 209.247.22.129 18:24, 24 April 2007 (UTC)
C retains water vapour well. If was dried out (cooking over mild heat) this probably wouldn't have happened
anyone who cuts coke with K and thinks they'll get away with it is a damn fool.
This is completely irrelevant. Wikipedia is probably not the best forum for advice on proper use and adulteration of illegal drugs. Drake144 (talk) 07:44, 15 October 2010 (UTC)
Too many templates!
This page is appearing at Category:Pages where template include size is exceeded - which means it cannot display all the templates included. Near the end of the source code you will see
<!-- NewPP limit report Preprocessor node count: 84893/1000000 Post-expand include size: 2048000/2048000 bytes (*) Template argument size: 1493785/2048000 bytes Expensive parser function count: 19/500 -->
The (*) item shows the problem. The only way to improve the page rendering is to remove unnecessary templates (or subst them) Ronhjones (Talk) 00:42, 29 December 2010 (UTC)
- The bottom navboxes have been using 77% of the post-expand limit, as most of 2 megabytes of formatted text. Another large template, {{Citation/core}} has used another 20% of the limit (in {Cite_web}, {Cite_news}, etc.). However, expensive parser functions are used by "tiny" {{Citation needed}} as [citation needed] and {{Page needed}} as [page needed] which were formerly tiny templates. Because the navboxes have been the largest resource drain, I linked them as navpages at the bottom, instead, as a table of titles:
- Related navpages:
- {{Depressants}}
- {{Hallucinogens}}
- {{General anesthetics}}
- {{Analgesics}}
- {{Antidepressants}}
- {{Neurotoxins}}
- {{Cholinergics}}
- {{Dopaminergics}}
- {{Opioids}}
- {{Glutamatergics}}
- Related navpages:
- However, even though the navboxes have been huge, those other templates need to be modified to not hog resources, as well. Outside this article, the Template:Citation/core should be changed to be 5x-10x times smaller. Plus, {Citation needed} or {Page needed} should be simplified to not use an "expensive parser function" - they are both an unbelievable 4x (not just double or triple, but 4 times) the size of a complex {Convert} calculation which determines numeric precision, deduces the output unit, calculates 13-digit accuracy, and rounds results to match plus wikilinks, with typesetting. Yes, {Citation needed} and {Page needed} together are 8x times the size of using {Convert} with its most complex settings. -Wikid77 (talk) 07:55, 4 January 2011 (UTC)
Ketamine biliopathy
PMID 19197097 indicates a biliary problem similar to the bladder-related complications of chronic ketamine use. Possibly not ready for prime time, but something to watch. JFW | T@lk 19:50, 9 February 2011 (UTC)
Source
You know.... most of the illegal K that is being used on the street right now is from India. This article doesn't mention India, and it should. —Preceding unsigned comment added by 75.160.18.241 (talk) 05:55, 22 April 2010 (UTC)
Well provide some verifiable sources and edit the article yourself. I presume you mention india because you have heard about it from a verifiable source. 86.176.190.93 (talk) 04:52, 2 July 2011 (UTC)
Methoxetamine
I'm concerned about this article. I started this article about Ketamine years back. I'm now looking at it I see no talk about MXE being an anolog of ketamine. Can we put this on there somewhere? Trust me, MXE is ketamine lol
ALSO! FUN FACT! Analog drug laws only pertain to schedule one and schedule two drugs. Since Methoxetamine is a research chemical of Ketamine, which is a SCHEDULE THREE DRUG, it is %100 LEGAL to possess and to sell FYI & FTW! BUY IT ON THE WEB. PAY WITH A CREDIT CARD - LEGALLY! LOL!
First, you're contradicting yourself by asserting that MXE is both ketamine and an analog of ketamine. I do agree with you, however, that this article would benefit from at least a mention of ketamine analogs, perhaps under the Recreational Use section, or even under Chemistry (with a link to the arylcyclohexylamine page). (Pmillerrhodes (talk) 20:41, 28 December 2011 (UTC))
Ketamine#External links section added
I've added Ketamine#External links. Any disputes? More links dealing with the medical use of ketamine could be added, as the current list deals mostly with its nonmedical use. Pmillerrhodes TalkUser 21:03, 2 January 2012 (UTC)
- I trimmed it a bit. There's still a great deal of redundancy with the links themselves as well as information in the article, which suggests more trimming would be appropriate. --Ronz (talk) 21:59, 2 January 2012 (UTC)
- Good call. The Merck Manual: Ketamine seems like a very good resource for ketamine's medical use; I will include it if there is no objection here. Pmillerrhodes TalkUser 23:22, 2 January 2012 (UTC)
"Nomenclature" to "Slang terms"
Most of Ketamine#Nomenclature seems repetitive, as the brand names and CI-581 appear in other places in the article. This section should be abridged to include only slang terms of Ketamine. I will make this change if there are no objections. Pmillerrhodes TalkUser 21:16, 2 January 2012 (UTC)
The section has been abridged. The following slang terms remain unsourced: "Kezzle", "Pony Powder", "Donkey Dust", "Tranx", "Horsey", "Ney", "Calvin Klein", and "CK One". (The last two referring to ketamine + coke.) Can anyone find any decent references for these? Pmillerrhodes TalkContrib 19:06, 3 January 2012 (UTC)
- Inserted reference for "Calvin Klein" and "CK1" Pmillerrhodes TalkContrib 04:04, 6 January 2012 (UTC)
Reorganization? and Ketamine#Pharmacology...
Some ideas for further revision:
- Reorganize the current content per WP:PHARMMOS
- Ketamine#Recreational use, Ketamine#Nonmedical use (under Ketamine#History), and Ketamine#Slang terms should be combined under a new section titled "Society and culture"; further, "Legal status" and "International brand names" could go under this new section as well
- Ketamine#Experimental antidepressant use, Ketamine#Treatment of addiction, and Ketamine#Complex regional pain syndrome could be combined under a new section "Research" as they describe experimental uses and not current practices
Also, with regard to Ketamine#Mechanism of action
- Ketamine#Mechanism of action requires editing regarding its focus on HCN1 channels per WP:UNDUE; further, muscarinic receptors are mentioned in the lead, but not in Ketamine#Mechanism of action
- Ketamine#Mechanism of action lacks references
Can anyone else weigh in on this? I'm more looking for what people think of reorganizing the article. Pmillerrhodes TalkContrib 20:51, 6 January 2012 (UTC)
- I've reworked Ketamine#Mechanism of action to make its contents more relevant to its clinical use (analgesia) and to reduce the number of single, animal studies cited in preference for (mostly) recent reviews per WP:MEDRS. The images demonstrating ketamine's stereoisomerism were retained. Pmillerrhodes TalkContrib 00:59, 10 January 2012 (UTC)
History/Recreational - Raves? Club Drug?
In the history section, the article states:
The incidence of recreational ketamine use increased through the end of the century, especially in the context of raves and other parties
I'm not sure this is entirely accurate. I think that the majority of 'recreational' use of Ketamine is in private settings; the effects of the drug at higher doses are not at all conducive to use in public settings. (It is, after all, an anesthetic.) I believe the Ketamine/Rave link is more significant in the UK, especially in the present, due to the differences in legality of Ketamine in the UK vs. the US. Either way, I think characterizing Ketamine as a "Club Drug" is somewhat innacurate. I believe the wording should at least be softened, perhaps to something along the lines of:
The incidence of recreational ketamine use increased through the end of the century, partially due to an increase in its popularity in the context of raves and other parties.
--Overand 00:14, 11 February 2006 (UTC)
- I've rewritten Ketamine#History; I believe it now accurately (albeit briefly) describes ketamine's emergence as a club drug, despite its anesthetic properties. Further expansion of Ketamine#History is forthcoming. Pmillerrhodes TalkUser 04:49, 2 January 2012 (UTC)
Reverted Ketamine, as stated in a poll by 60% of highschoolers across America, is the most accessable and mind-clearing drug. It's absolutely amazing! 32% can't live without it. --Dakota ~ ° 23:31, 17 February 2006 (UTC) ketamine is a cure for comedowns from ecstacsy.
o_O Where are all of these highschoolers getting Ketamine? I have yet to find any source for it. Most people I know haven't even heard of it. 209.247.22.129 18:25, 24 April 2007 (UTC)
- Good question. As an "old man" now, I can't find squat... but I will say that one as-yet-unmentioned use for the drug is to also mediate comedown from LSD. After a whole night of doing [-[:UNKNOWN:]-], it can sometimes literally hurt to return to normality. A single small bump of K will perform the miraculous: bring back the visuals, take away any pain, and help you finally get to bed. (But should only be used in those amounts, and only once you're really "grounding". Don't be greedy!) Pimpoosh (talk) 18:25, 30 May 2012 (UTC)
Common Street Slang
I have revised the street slang to provide a source for all of the current terms. Future terms added to the article should add their own source to the header, such as: The GDCADA and Group XYZ give the following common street slang terms for ketamine.... ju66l3r 04:32, 10 February 2007 (UTC)
- Fantastic; Im glad you've found a source. I've considered ditching that section a few times. John Vandenberg 05:32, 10 February 2007 (UTC)
- I happened to come looking it up because of a rerun of South Park's "Little Whore Playset" spoof on Paris Hilton (the girls in town were going to have a rave party and take Ketamine, even though they didn't know what it was). I was pretty sure it was also known as Special K and the section looked like about 50% vandalism or neologism and 50% truth, so I went source hunting. Glad to help...I also feel pretty strongly about these half-baked lists like "slang" or "trivia" or "cultural refs" that don't come with any sourcing for verifiability. I usually try to wipe them when I can, but I figured someone somewhere had to have a page on Learn what you kids are talking about or similar when it came to a street drug. ju66l3r 06:37, 10 February 2007 (UTC)
- Ju66l3r's version of a well sourced "#Common_Street_Slang" section was recently removed by Cacycle (talk · contribs), with a decent enough reason. However, when asked a real question that required I refer to this list, I find it is effectively gone, so I am a bit miffed. I'll get over it and bookmark the old version, but what do others think? John Vandenberg 11:27, 20 June 2007 (UTC)
- Wikipedia is not a slang guide for good reasons, please see Wikipedia:What Wikipedia is not#Wikipedia is not a dictionary and Wikipedia:Wikipedia is not a dictionary. However, there are links to sites that list list such slang names in the article and you might want to check Wiktionary. The problem is that there is usually no reliable source about where, when, and by whom these names were actually used (the reference [5] was definitely not a reliable source in this context). Most slang terms are temporarily and spatially restricted, often to very small groups or circles of friends. Cacycle 20:26, 20 June 2007 (UTC)
- Nor is Wikipedia a place for singular crusades by overbearing elitists. The VAST MAJORITY of information here is "tempor[AL]ly and spatially restricted" - that's the POINT of a knowledge repository. If it was common knowledge, why would all of us bother? Street slang is a core facet of the use of illicit substances, and these are ABSOLUTELY NOT simply dictionary synonyms. Try writing a research paper titled "Casey and its effects" or "Neurotoxicity Study for users of Mary Jane". So.... not quite. As to reliable source, there are a great many reasons to countermand the dismissal of questionably-sourced info such as this, particularly given the utter impossibility of obtaining such when combined with the very real needs of wishing to refer to such information (QED Jayvdb). This is not a binary issue, and if you will insist it is (which I feel is a perversion of the spirit of wikipedia), then the guidelines need to be refined around this very gray edge, because it is many times more useful to include a section with heavy qualifications owing to the Singularly Unique circumstances of the lack of scholarly verifiability of the details of illicit activity, than to excise it outright and force others to look elsewhere, which rather completely eliminates the point of an encyclopedia. I've yet to read a single article in the Brittanica that mentions "why not check Webster's?" anywhere. Parthian Shot: Miswordings like "temporarily" do much to undermine your perceived authority, while simultaneously enforcing the perception of you hiding behind the overbearing power of bureaucracy. I am responding here through benefit of the doubt. I also suspect this will never get read, but hey, wtf. It needed saying. Pimpoosh (talk) 18:53, 30 May 2012 (UTC)
- It is also called Kelly or Kelly Osbourne as a street name due to avoid detection i.e. "Is Kelly coming to the party", also I'm lead to believe this is due to Ms Osbourne's very white appearance.gherks 22:16, 19 August 2007 (BST)
Antidepressant properties
The fast-acting antidepressant potential of ketamine has been significantly, although not wholly, characterized in recent years; yet, the current version of this article fails to reflect this. A short search in PubMed reveals the following review articles (all published in 2012 alone) regarding ketamine's antidepressant potential: [6], [7], [8], [9], [10]
Given the media attention ketamine has received as of late, a re-write of this section seems necessary. Pmillerrhodes TalkContrib 19:23, 21 August 2012 (UTC)
Toxicity, Prevention, Pharmacology
Toxicity with ketamine is partially a dose dependent phenomenon. In rats and the rhesus monkey, doses of severe magnitude caused damage at excitatory synapses in the hippocampus of the brain after a matter of hours. At anesthetic and subanesthetic doses ketamine functions as a neuroprotective agent. Adjunctive medications are available to mitigate any potential toxic side effects, and they included agents which function as: an alpha-2-adrenogenic agonist, a 5HTA1 agonist, a GABA-A agonist, as well as a H1 antagonists. Ketamine does not directly cause any harm through its blockade of NMDA and glutamate, in fact that aspect is highly neuroprotective. While the primary effects of ketamine did not cause any damage to the brain, the Post-acute-withdrawal following a large dose, especially an intravenous dose, causes a rebound effect at the receptor site- in this case increasing endogenous glutamate and quinonolic acid/NMDA [GluR receptor agonists]1.
This type of toxicity causes eventual neuronal apotosis and lipid peroxidation, and has been documented in studies with both rats2 and the rhesus monkey3. The study requires killing the test subject and examining the brain directly through dissection and enzymatic testing, thus preventing the test to be run on humans. This type of brain cell death is and toxicity is most similar to the progression of Huntington’s disease, but also bears similarity such as the same cell death pathway as dementia caused by Alzheimer’s disease. For cell death to occur the magnitude or frequency of dosage must be high, since the imbalance must be sustained for damage to occur. Behavioral effects to be observed for quinolinic acid toxicity (an endogenous NMDA agonist) include a marked increase in circling behavior. This was initially noted for tests with rats but circling is a behavior prevalent in most (if not all) mammals including rats, cats, dogs, monkeys, and humans.
The damage is actually caused directly by elevated extracellular glutamate levels, a scenario which has been replicated in many studies. At these high concentrations glutamate activates the extrasynaptic NMDA receptor, which sends a cascading signal to kill surrounding neurons. [often referred to as the glutamate storm]
One hypothesis is that the mechanism for this may be a sort of endogenous measure for the body to protect itself from certain types of neuro-poisons, by eliminating the affected tissue before it has a chance to spread- although that still remains unclear and further research may be warranted.
Research has also uncovered another element in the system, namely the role of phospholipase C in NMDA and glutamate neurotoxicity. Inhibition of this enzyme contributes neuroprotective effects of its own4. Other compounds exert similar inhibition over phospholipase C including the anti-cancer5,6 phytocannabinoid cannabidiol7 (CBD)7 as well as the endocannabinoid 2-arachidonyl glycerol7. Interestingly, CBD also functions as a 5HTA1 agonist, as well as an alpha-2-adrenogenic agonist, making it an ideal adjunctive medication for use with ketamine. Supplementation of magnesium, B-12, B-6, and folate would also help balance out the equation, especially if ketamine is to be administered on any type of regular basis. An after-effect of ketamine is also an Increase in the [Ca2+ : Mg2+] ratio, which is essentially the logic gate by which glutamate functions, via depolarization. The result of which is a shift in equilibrium from neutral to agonistic, which if persists, causes neuronal damage and eventually brain-cell death. Since calcium regulate glutamergic agonistic function, and glutamate receptors are the most abundant excitatory neurotransmitter in the brain, its impact is widely felt. The increase will also increase THC’s (CB1 agonist) effectiveness, whilst decreasing CBD’s (CB1 antagonist, CB2 agonist) effectiveness. The imbalance at that receptor complex can be attenuated via potassium supplementation [cannabinoid agonist activity=Ca2+, cannabinoid antagonist activity=K+].
{Mg offsets the Ca imbalance, B-6 assists in adrenogenic function since that system is stressed (amphetamine ring), and B-12 assists the body with the increase production of melatonin. Mg + B6 also help with the conversion of excess glutamate into GABA, as well as 5-HTP into serotonin, concentrations of which are naturally neuroprotective against glutamergic toxicity. Extracellular levels of GABA are increased during and following treatment with ketamine11, something which helps differentiate ketamine and PCP, as phencyclidine does not exhibit this feature11. That, in addition to PCP being an arylcyclohexylamine with an unmodified phenyl group as its aryl substituent (which imparts it with the ability to inhibit dopamine uptake14 and increase dopamine efflux14, which it does much more aggressively than the S(+) isomer of ketamine.) [ketamine has o-chlorophenyl as its aryl substituent, which is a modified phenyl.]} Ketamine’s effect profile can be further removed from PCP if taken in conjunction with an alpha-2-adrenogenic agonist such as clonidine HCl. This blocks excitation at the norepinephrine and epinephrine (adrenaline) receptors, thus negating any remaining excitatory amphetamine qualities.
Other compounds which can exert protective effects from this specific type of toxicity achieved as a rebound from prolonged or consistent ketamine administration include 7c-KYNA and AP-7 (the former of which is thought to contribute significantly to heated milk’s anxiolytic profile, in addition to tryptophan) as they are glycine site modulation blockers and NMDA recognition site blockers, respectively.8 Amphetamines, MSG, aspartame, seaweed (kainic acid content), and excess calcium supplementation can exacerbate, or even cause in their own right, neuronal (glutamergic) toxicity in the brain. Kainic acid also increases seizure risk from strobe lights (regulates light input to the brain). Ketamine should not be combined with monoamine oxidase inhibitors nor phosphodiesterase inhibitors [diazepam, Viagra] due to potential unrelated toxicity. Agents that inhibit hepatic CYP enzymes [bermagottin(in grapefruit), and several SSRI class medications and barbituates] should be carefully researched first as they may cause an aversive reaction, such as impeding the body’s ability to break down the compound, exacerbating plasticity issues, or creating them where they don’t already exist.
This type of toxicity is not new; benzodiazepines do the same thing, except they do it on the GABA-A receptor instead of the NMDA receptor- which is the chemical explanation for rebound anxiety occurring upon discontinuation of a benzodiazepine. It is a natural part of tolerance and plasticity, and can be mitigated like many side effects, but only if it is acknowledged first. Ketamine is actually quite safe and of great medical value if used correctly, but as with all things if misused it can be dangerous. **DO NOT OPERATE MACHINERY UNDER THE INFLUENCE OF KETAMINE** Ignoring rebound plasticity or repeatedly increasing dosage to achieve previously achieved dopamine euphoria are only real ways to misuse ketamine, but both seem fairly prevalent amongst uninformed recreational users. The latter can be fixed by using the R(-) stereoisomer of ketamine, since it is identical in every way to its S(+) except in terms of dopamine efflux and dopamine uptake inhibition. [S(+)ketamine causes an increase in dopamine efflux as well as an uptake inhibition(approx100% increase). Racemic ketamine exhibits a dopamine release which becomes attenuated after 7 days. R(-)ketamine had no effect on S(+)ketamine’s dopamergic transmission. Deductively the dopamergic transmission of S(+)ketamine alone must attenuate over a 7 day period of continued, constant-dose administration, since the racemic mixture [50% S(+)ketamine, 50% R(-)ketamine]produced the same results, and later experiments proved R(-)ketamine to not be an active participant in dopamergic transmission, nor a modulator of S(+)ketamine’s dopamergic transmission. Arguably R(-)ketamine could be made in an oral or sublingual tablet which could be rescheduled as a Schedule IV drug due to its lack of dopamine, the main euphoric neurotransmitter associated with addictive disorders. S(+)ketamine and racemic mixtures containing 35% or more S(+)ketamine in ratio to R(-)ketamine would remain Schedule III since the release of dopamine makes the compound more euphoric, and the rapid attenuation of dopamine increases the likelihood of compulsive increases in doses amongst recreational users. Lack of physical addiction prohibits its placement in Schedule II. Currently all forms of ketamine are Schedule III in the United States.
Additionally since ketamine not only achieves GABA site modulation and instigates a plasticity reduction at the site, but also effectively blocks the transmission of the Nicotinic acetylcholine receptors9, it may be a highly useful adjunctive in the treatment of both alcohol and cigarette addiction. The GABA site modulation and plasticity reduction provides an anxiolytic effect while the nicotinic channel blocking would block that aspect of nicotine and alcohols effect. (Patient would still be able to ascertain a sense of euphoria from dopamine uptake inhibition and oxygen deprivation from cigarette smoking, but nACH blocking should inhibit a percentage of compulsions for another cigarette if they are ready to attempt quitting.) It should be marginally to moderately more effective as a treatment for alcohol abuse than nicotine/carbon monoxide abuse, since GABA is considered the major chemical responsible for alcohol cravings, whereas the nicotinic acetylcholine is responsible partially for the energy and racing thoughts associated with intoxication on ethanol.
A H1 histamine antagonist would prove useful against a rush of excitatory histamine, since activation of the D2 and D3 dopamine receptors results in a surge of histamine10- much the same way as metamphetamine.10 This should also provide another layer of inhibitory support, and is why anticholinergic class drugs are often recommended as an adjunct to ketamine.
Ketamine also causes an output of melatonin, a quality that other anesthetics such as pentobarbital and halothane do not share.12 Such an action depletes available folic acid, and therefore individuals with low levels of folic acid may experience a greater disturbance of sleep patterns than an individual with an ample supply. It also may lend an effect in its usefulness as an antidepressant agent. Subsequent research found that subeffective doses of melatonin [0.001mg/kg] in conjunction with ketamine provided a synergistic effect13 amplifying its anti-depressant action. The synergistic effect also occurred with MK-80113 and zinc chloride13, fellow NMDA antagonists.
Abbreviations
5HTA1 a subtype of serotonin (5-HT) receptor
GABAA a subtype of GABA receptor
H1 a subtype of the histamine receptor
GluR Glutamate receptor site complex
CB1 a subtype of cannabinoid receptor
CB2 a subtype of cannabinoid receptor
CBD cannabidiol (non-psychoactive, sedative, anti-tumor agent, the degradation product of THC)
THC delta-9-tetrahydrocannabinol (psychoactive component of cannabis)
S(+) refers to dextrorotation and levorotation in stereoisomers
R(-) refers to dextrorotation and levorotation in stereoisomers
KYNA kynurenate / kynurenic acid (part of tryptophan’s degradation pathway)
7-cKYNA[derivative of KYNA], 7-chlorokynurenate (an NMDA glycine site antagonist)
AP-7 2-amino-7-phosphonoheptanoate (a NMDA recognition site blocker)
nACH Nicotinic Acetylcholine
5-HTP 5-hydroxy-tryptophan [an intermediate metabolite between tryptophan and serotonin]
MK-801 a noncompetitive NMDA antagonist, Dizocilpine.
Kainic acid a type of glutamate receptor agonist that binds to a glutamate insensitive site- Deals with processing light input in the brain and is present in goldfish and humans.
Sources
1] J. F. William Deakin, PhD, FRCPsych, FmedSci; Jane Lees, BSc, MSc; Shane McKie, MEng, MSc, PhD; Jaime E. C. Hallak, MD, PhD; Steve R. Williams, BA, MA, DPhil; Serdar M. Dursun, MD, PhD, FRCPC. "Glutamate and the Neural Basis of the Subjective Effects of Ketamine." A Pharmaco-Magnetic Resonance Imaging Study. Arch Gen Psychiatry. 2008;65(2):154-164 http://www.rsds.org/pdfsall/Deakin_Lees_McKie.pdf (alternative location listed in proceeding link.) https://docs.google.com/viewer?a=v&q=cache:wu_UHtLbMekJ:www.rsds.org/pdfsall/Deakin_Lees_McKie.pdf+&hl=en&gl=us&pid=bl&srcid=ADGEESj5CXX5Mr69E46jmL59BgmNyr_rqTzdTgf6iaK8WpjVLsakbuPnli28uh0wLqC-IhpgOM8NHQgxGcAOTqugWe4QJdTti0W0xREdYI-mC0a5sQ_W4gkCnzWlgQiEsE1hq9r-hACI&sig=AHIEtbSXzLPJz0WU0VjmePQji1bURNwueg&pli=1
2] “Protective effects of the antioxidant selenium on quinolinic acid-induced neurotoxicity in rats: in vitro and in vivo studies.” Santamaría A, Salvatierra-Sánchez R, Vázquez-Román B, Santiago-López D, Villeda-Hernández J, Galván-Arzate S, Jiménez-Capdeville ME, Ali SF. Departamento de Neuroquímica and Neuromorfología Celular, Instituto Nacional de Neurología y Neurocirugía Manuel Velasco Suárez, Mexico City, Mexico. J Neurochem. 2003 Jul;86(2):479-88. PMID: 12871589 http://www.ncbi.nlm.nih.gov/pubmed/12871589
3] “Brain lesions in an infant rhesus monkey treated with monsodium glutamate.” Olney JW, Sharpe LG. Science. 1969 Oct 17;166(3903):386-8 PMID: 5812037 http://www.ncbi.nlm.nih.gov/pubmed/5812037
4] “Inhibitors of Phospholipase C Prevent Glutamate Neurotoxicity in Primary Cultures of Cerebellar Neurons” Marta Llansola, Pilar Monfort and Vicente Felipo Instituto de Investigaciones Citologicas, Fundación Valenciana de Investigaciones Biomédicas, Valencia, Spain The American Society for Pharmacology and Experimental Therapeutics JPET March 1, 2000 vol. 292 no. 3 870-876 http://jpet.aspetjournals.org/content/292/3/870.abstract
5] http://www.cancer.gov/cancertopics/pdq/cam/cannabis/healthprofessional/page4 [National Cancer Institue, part of the National Institute of Health (NIHA)]
6] Aviello G, Romano B, Borrelli F, et al.: “Chemopreventive effect of the non-psychotropic phytocannabinoid cannabidiol on experimental colon cancer.” J Mol Med (Berl) 90 (8): 925-34, 2012. [PUBMED Abstract] [CBD specific article used in Reference 5, given for specicifity.]
7] “Interactions of cannabidiol with endocannabinoid signalling in hippocampal tissue.” Ryan D, Drysdale AJ, Pertwee RG, Platt B. School of Medical Sciences, College of Life Sciences and Medicine, University of Aberdeen, Institute of Medical Sciences, Foresterhill, Aberdeen AB25 2ZD Scotland, UK. Eur J Neurosci. 2007 Apr;25(7):2093-102. PMID: 17419758 http://www.ncbi.nlm.nih.gov/pubmed/17419758
8] “Quinolinic acid, the inescapable neurotoxin.” Guillemin GJ. Department of Pharmacology, School of Medical Sciences, University of New South Wales, Sydney, NSW, Australia. g.guillemin@unsw.edu.au FEBS J. 2012 Apr;279(8):1356-65. doi: 10.1111/j.1742-4658.2012.08485.x. Epub 2012 Mar 27.
9] “Nonstereoselective inhibition of neuronal nicotinic acetylcholine receptors by ketamine isomers.” Sasaki T, Andoh T, Watanabe I, Kamiya Y, Itoh H, Higashi T, Matsuura T. Department of Anesthesiology, Yokohama City University School of Medicine, Japan. Anesth Analg. 2000 Sep;91(3):741-8. PMID: 10960411 http://www.ncbi.nlm.nih.gov/pubmed/10960411
10] Jean-Charles Schwartz, Jean-Michel Arrang. Neuropsychopharmacology: The Fifth Generation of Progress. Chapter 14: Histamine 187 "Histamine, Schizophrenia, and Antipsychotic Drug Actions". Edited by Kenneth L. Davis, Dennis Charney, Joseph T. Coyle, and Charles Nemeroff. American College of Neuropsychopharmacology (C) 2002. http://www.acnp.org/asset.axd?id=92f0f055-db49-41dd-880d-10d5a5bbf5b6 (direct link to chapter 14- histamine) http://www.acnp.org/publications/neuro5thgeneration.aspx (link to table of contents, with all chapters available) {Source’s reference: [77,78]}
11] “Ketamine, But Not Phencyclidine, Selectively Modulates Cerebellar GABAA Receptors Containing α6 and δ Subunits” Wulf Hevers1,3, Stephen H. Hadley2, Hartmut Lüddens1, and Jahanshah Amin2 - Author Affiliations 1Carl-Ludwig Department of Physiology, University of Leipzig, D-04103 Leipzig, Germany, 2Department of Molecular Pharmacology and Physiology, University of South Florida, Tampa, Florida 33612, and 3Laboratory of Molecular Biology at the Department of Psychiatry, University of Mainz, D-55131 Mainz, Germany The Journal of Neuroscience, 14 May 2008, 28(20): 5383-5393; doi: 10.1523/JNEUROSCI.5443-07.2008 http://www.jneurosci.org/content/28/20/5383.abstract
12] “Effects of Halothane, Pentobarbital and Ketamine on Serum Melatonin Levels in the Early Scotophase in New Zealand White Rabbits” Celia S. Panga,b, Charlotte Mulniera, Shiu F. Pangb, Joseph C.S. Yanga. Author affiliations [a]Department of Anaesthesiology, [b]Department of Physiology, University of Hong Kong, Hong Kong. Biol Signals Recept 2001;10:310-316 (DOI: 10.1159/000046898) Vol. 10, No. 5, 2001 http://content.karger.com/ProdukteDB/produkte.asp?Aktion=ShowFulltext&ArtikelNr=46898&ProduktNr=227443
13] “Melatonin exerts an antidepressant-like effect in the tail suspension test in mic: evidence for involvement of the N-methyl-D-aspartate receptors and the L-arginine-nitric-oxide pathway.” Michela Mantovani a, Roberto Pe ´rtile a, Joa ˜o B. Calixto b, Adair R.S. Santos c, Ana Lu´cia S. Rodrigues a, *a Departamento de Bioquı´mica, Centro de Cieˆncias Biolo´gicas, Universidade Federal de Santa Catarina, Floriano´polis, SC 88040-900, Brazil b Departamento de Farmacologia, Centro de Cieˆncias Biolo´gicas, Universidade Federal de Santa Catarina, Floriano´polis, SC 88040-900, Brazil c Departamento de Cieˆncias Fisiolo´gicas, Centro de Cieˆncias Biolo´gicas, Universidade Federal de Santa Catarina, Floriano´polis, SC 88040-900, Brazil. Neuroscience Letters 343 (2003) 1–4. http://www.landi.ufsc.br/Artigos/2003/2.Mantovani%20et%20al.Neuroscience%20Letters.PDF
14] “Role of the aromatic group in the inhibition of phencyclidine binding and dopamine uptake by PCP analogs” Isabelle Chaudieua, ∗, Jacques Vignona, ∗, Michèle Chicheportichea, ∗, Jean-Marc Kamenkaa, ∗, Gérard Trouiller∗, Robert Chicheportiche , a, ∗ ∗ CNRS LP 8402, INSERM U 249 (UMI), Laboratoire de Biochimie Ecole Nationale Supérieure de Chimie de Montpellier, 8 rue de l'Ecole Normale 34075 Montpellier Cedex, France b Service de Pharmacologie, Centre d'Etude du Bouchet, BP 3, 91710 Vert Le Petit, France http://dx.doi.org/10.1016/0091-3057(89)90020-8 Pharmacology Biochemistry and Behavior Volume 32, Issue 3, March 1989, Pages 699–705 http://www.sciencedirect.com/science/article/pii/0091305789900208
"Oral ketamine is more potent than SC ketamine (due to liver metabolism)"
This is presented as if self-evident but to me it is not: if liver metabolism is important, first pass metabolism of ketamine in the portal venous blood would reduce plasma drug levels after oral administration, an effect absent with parenteral dosing. If oral ketamine really is more potent than subcutaneous then that would be remarkable and would invite a rational explanation. Moletrouser (talk) 19:16, 3 February 2013 (UTC)
I wouldn't be surprised if that was just a typo and the writer intended to say the opposite. Exercisephys (talk) 21:26, 3 February 2013 (UTC)
Claimed use in Mali
The single French-language source for this claim may be problematic, as it seems largely based on rumour/supposition, and even the accompanying photograph claiming "syringes" actually shows IV cannulas. I'm removing it, until such time as someone can come up with some more robust sources. Nick Cooper (talk) 17:11, 24 February 2013 (UTC)