Talk:Nicotine/Archive 2
| This is an archive of past discussions about Nicotine. Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |
| Archive 1 | Archive 2 |
Lede edits
Quackguru, you made edit, saying "tighten lede and remove SYN violation and move content to body and rewrite claim to avoid SYN violation; see to verify claim: "Though nicotine replacement therapy is less harmful than tobacco, nicotine by itself is associated with its own health problems, notably cancer, cardiovascular disease, birth defects (possibly), and poisoning." "
You took "The general medical position is that nicotine itself poses few health risks, except among certain vulnerable groups[1] such as young adults.[2]" and removed the second clause. Since almost all the people becoming addicted to nicotine are adolescents and young adults, this is highly relevant, and should be in the lede. Using two sources to support two different clauses is not WP:SYN. You moved this content lower in the article, writing "Adolescents seems to be vulnerable to the negative effects of nicotine on the central nervous system." The source lists serious long-lasting mental harms for both adolescents and young adults. There is evidence that teenagers do not identify as adolescents, so just listing adolescents seems like a bad idea, and being vague about the harms is also a bad idea.
If the source says "nicotine by itself is associated with its own health problems, notably cancer, cardiovascular disease, birth defects (possibly), and poisoning", why does the article say only "Nicotine is linked to possible birth defects"? I have some better sourcing for birth defects, will add. HLHJ (talk) 18:13, 28 October 2018 (UTC)
- The lede is getting too long and I moved text to the body and rewritten it. The article says "Nicotine is linked to possible birth defects" and goes into detail using other sources for content about nicotine in the body. QuackGuru (talk) 18:29, 28 October 2018 (UTC)
- The lede is too long, but it also has serious omissions. HLHJ (talk) 23:33, 28 October 2018 (UTC)
- When the lede is too long content can be moved to the body. I'm not sure what else can be summarised in the lede. For a complex article there will always be omissions. The extraneous details can be expanded in the body. QuackGuru (talk) 08:23, 29 October 2018 (UTC)
- The lede is too long, but it also has serious omissions. HLHJ (talk) 23:33, 28 October 2018 (UTC)
OK, so, speaking of "the lede", Nicotine is a potent parasympathomimetic stimulant and an alkaloid found in the nightshade family of plants.[4] Nicotine acts as a receptor agonist at most nicotinic acetylcholine receptors (nAChRs),[5][6] except at two nicotinic receptor subunits (nAChRα9 and nAChRα10) where it acts as a receptor antagonist.[5] Nicotine is found in the leaves of Nicotiana rustica, in amounts of 2–14%; in the tobacco plant, Nicotiana tabacum; in Duboisia hopwoodii; and in Asclepias syriaca.[7] ...has anyone considered starting the article with something other than incomprehensible jargon? Why is "parasympathomimetic" in the first sentence? Why is "nicotinic receptor subunits" in the first paragraph that Google picks up for its summaries? et cetera. -2406:5A00:C003:3F00:C09A:59A8:E85D:CA5A (talk) 06:12, 16 November 2018 (UTC)
- I moved all of the content on what plants nicotine is found in and in what concentrations it is found into a "sources" section, and instead mentioned in the lede that nicotine is addictive, and has certain health effects. I strongly think that a separate section on sources of nicotine would be preferable to spending a third of the lede listing botanical sources. QuackGuru, you reversed these changes, with an edit comment "update lede and body; please redo any edits you think need to be redone". Some of the changes you made seem to me to be contrary to consensus in this discussion, in which you participated. I think that they muddy the phrasing of the information; for instance, you replaced, "At high-enough doses, nicotine is poisonous" with "At high-enough doses, it is associated with nicotine poisoning", sticking a referent with no ancedent at the beginning or a paragraph. While it is quite difficult to read through your changes, and I may have overlooked some valuable improvements, I think I prefer the previous version.
- More worryingly, you seem to have removed bibliographic information from sources that do not support a pro-e-cigarette point of view, specifically fulltext urls, PMC IDs, PubMed IDs, and page numbers, which give the reader easier access to original paper. While replacing these would be a minor edit, I don't want to trawl through articles replacing this information, especially as I think I recall inserting it before, often enough that I found myself wondering if my déjà vu was actually all in my head. I do not want to engage in an edit war over fulltext access links. Please replace any such bibliographic information that you have removed from any citations on Wikimedia projects. You also removed in-cite quotation text which I think I had added in response to your complaints about verification; I'd appreciate having that restored. HLHJ (talk) 04:59, 13 January 2019 (UTC)
- You made bold edits and I disagreed. Please start a RfC or wait for others to comment. Citation bot usally will can fix the citations. I'm not sure which ref you want me to fix. The in-cite quotation text is a distraction in the reference section for the reader and also unnecessary. QuackGuru (talk) 05:17, 13 January 2019 (UTC)
- More worryingly, you seem to have removed bibliographic information from sources that do not support a pro-e-cigarette point of view, specifically fulltext urls, PMC IDs, PubMed IDs, and page numbers, which give the reader easier access to original paper. While replacing these would be a minor edit, I don't want to trawl through articles replacing this information, especially as I think I recall inserting it before, often enough that I found myself wondering if my déjà vu was actually all in my head. I do not want to engage in an edit war over fulltext access links. Please replace any such bibliographic information that you have removed from any citations on Wikimedia projects. You also removed in-cite quotation text which I think I had added in response to your complaints about verification; I'd appreciate having that restored. HLHJ (talk) 04:59, 13 January 2019 (UTC)
- I'd like you to fix all the refs from which you removed bibliographic information that would help the reader access the fulltext easily. You removed the information on the 1st of January; Citation Bot has not fixed yet, so it seems unlikely that it will fix. This is why I asked that you fix it manually. HLHJ (talk) 05:37, 13 January 2019 (UTC)
- User:Boghog is currently redoing the citations.[2] It may be possible to ask for Citation Bot to edit the article. QuackGuru (talk) 05:55, 13 January 2019 (UTC)
- I'd like you to fix all the refs from which you removed bibliographic information that would help the reader access the fulltext easily. You removed the information on the 1st of January; Citation Bot has not fixed yet, so it seems unlikely that it will fix. This is why I asked that you fix it manually. HLHJ (talk) 05:37, 13 January 2019 (UTC)
- That's good of Boghog, but I think BogHog is doing citation formatting, not restoring access information. I think that it is your responsibility to restore it.
- You removed this section from the lede:
Nicotine dependency causes distress.[3][4] Nicotine withdrawal symptoms include depressed mood, stress, anxiety, irritability, difficulty concentrating, and sleep disturbances.[5] Mild nicotine withdrawal symptoms are measurable in unrestricted smokers, who experience normal moods only as their blood nicotine levels peak, with each cigarette. On quitting, withdrawal symptoms worsen sharply, then gradually improve to a normal state.[6]
- The lede now contains information on the mental/emotional effects of nicotine on animals, but not on nicotine-dependent humans. This seems odd. I'd like to restore this content; do you have any objection?
- You also moved the sentence "It is one of the most commonly abused drugs.[7]" to the end of the paragraph; can you tell me why? It formerly followed the sentence "Nicotine is highly addictive"; now it follows a sentence whose subject is nicotine dependence, making the referent nonsensical. HLHJ (talk) 06:15, 13 January 2019 (UTC)
- Not sure what citation verifies "Mild nicotine withdrawal symptoms are measurable in unrestricted smokers, who experience normal moods only as their blood nicotine levels peak, with each cigarette." For now I restored the content. I looked at the citations. I'm not sure what exactly needs to be restored for each citation. I think it would take too much time to go through each citation and compare each one. Eventually it will be fixed. There may be a way to trigger one of the bots to update anything that can be updated. QuackGuru (talk) 08:47, 13 January 2019 (UTC)
- You also moved the sentence "It is one of the most commonly abused drugs.[7]" to the end of the paragraph; can you tell me why? It formerly followed the sentence "Nicotine is highly addictive"; now it follows a sentence whose subject is nicotine dependence, making the referent nonsensical. HLHJ (talk) 06:15, 13 January 2019 (UTC)
- There were two sentences, followed by one citation which supported both. I've duplicated the citation and removed your cn tag. Thank you for restoring that content, and moving the dangling referent back.
- I would also appreciate it if you would restore the "sources" section, the information on why plants make nicotine at all, the information that young adults are more likely (indeed, in practice, almost the only people) to become nicotine-dependent, the information that nicotine from NRTs and e-cigarettes is well-documented to cause fetal harms, and other information you removed.
- It would also be good to clarify some of the content you added. For instance, what does "Pregnant women, breastfeeding mothers, and the elderly are more sensitive to nicotine than other individuals" mean in terms of concrete health outcomes? I think the sentence formerly at the start of that section was much clearer. Some phrasing seems so unclear as to hinder understanding; for instance: "It is hard to determine the long-term safety of nicotine"; the problem actually seems to be that there is only one medium-long-term (seven-year) study of the effects of nicotine in NRT form.[8] I thought I had inserted this information, but now can't find that version.
- You also replaced the statement "The general medical position is that nicotine itself poses few health risks, except among certain vulnerable groups"; I had explained in an edit comment that it was outdated, based on a 2007 source, and contradicted by more recent information and sources which I added. Could you please remove it again, and restore the information on what the health risks are?
- I'm sorry, QuackGuru, I don't want to be too down on you, but I didn't see anything really useful in your New Year's Day edits. Maybe you stayed up too late the night before?

- Finally, and most importantly, citations. The point of citations is to make it easy for the reader to assess and access the original sources of information. Fulltext links, catalogue links, and page numbers all assist in this process. The only halfway respectable reason I can think of for removing such information is if one's publisher insists on a rigid referencing format which will not accommodate it. Wikimedia is not such a publisher. It seems to me that removing such information unequivocally degrades the citation. I can't figure out why you thought (or possibly still think?) that removing this information improved the encyclopedia. Could you please explain what you were thinking? Have you ever done this anywhere else on Wikimedia projects?
- You are right to say that it will take a lot of time to go through each citation and compare each one, and restore the degraded citations. That is why I am asking you to do it. I think that it is your responsibility. HLHJ (talk) 00:55, 14 January 2019 (UTC)
- QuackGuru, on my talk page, you replied:
I don't have time to respond and edit for the nicotine page. I am busy. Maybe you can get feedback from others. I don't want to keep you waiting for me. I thought I give you a heads up. You can also start a RfC for other opinions. QuackGuru (talk) 01:48, 14 January 2019 (UTC)
- I will await comment from others. Could you please tell me if there are any other places where you have removed bibliographic information that would help the reader find the fulltext easily? HLHJ (talk) 01:59, 14 January 2019 (UTC)
- QuackGuru, I think I've done you an injustice. I was imagining you going through and removing all that bibliographic data by hand, which I should have immediately realized is not your style. It was really ridiculously dense of me not to realize that you'd just reverted to an earlier version, before this information was added by myself and others. I think you reverted, with modifications, to something like the version of the 14th of November, which was the last time you had edited the page. This effectively reverted a number of edits by myself and other editors, some of which were very gnomish. A revert from the 1st of January to the 14th of November is rather dramatic, especially when some of the intervening edits had consensus in a discussion in which you participated, albeit fairly peripherally. Your edit comment "update lede and body; please redo any edits you think need to be redone" does not give a clear idea of what you did. Next time, could you please use an edit comment something like "Reverted to version of 14:12, 14 November 2018 because of..."? This would avoid my asking you on the talk page why on earth you removed uncontroversial information like page numbers; it would be obvious.
- As there have been substantive edits to the article since, redoing the edits you undid seems to me as if it is going to involve manual merging. As you say, this will take a lot of time. I ask that you take this time, or explain why you will not. HLHJ (talk) 18:30, 14 January 2019 (UTC)
- QuackGuru, I got consensus for some content, and shortened the lede at your suggestion. You reverted a month and a half of edits by multiple editors, on the first of January. When I asked you to undo that very bold edit, you said you did not have time to do that or to discuss the changes. Do you object to my manually undoing your New Year's Day edits myself? HLHJ (talk) 03:13, 5 February 2019 (UTC)
- See this comment about my edit. Seppi333 did not object to my edit. Seppi333 shortened the lede a bit. You drastically changed the lede. The lede should stay 4 paragraphs IMO.
- See Nicotine#Occurrence_and_biosynthesis for the Sources section. The lede summaries that section. It should not be moved to the body and have duplicate sections. I said I did not have time to manually update the citations. It was not about my edit. I think you misunderstood me. I objected to your bold changes. Seppi333 made a lot of recent changes to this article and redid his edits. @Seppi333: should also be asked about the changes you want to make or you can start a RfC. It would not be fair to Seppi333 to make drastic changes to this article after he cleaned up the article. You can also create a draft page and seek input. QuackGuru (talk) 16:20, 5 February 2019 (UTC)
- QuackGuru, I got consensus for some content, and shortened the lede at your suggestion. You reverted a month and a half of edits by multiple editors, on the first of January. When I asked you to undo that very bold edit, you said you did not have time to do that or to discuss the changes. Do you object to my manually undoing your New Year's Day edits myself? HLHJ (talk) 03:13, 5 February 2019 (UTC)
- I agree that the lede is too long, but that's a side issue. I'm talking about a large revert including some of Seppi333's own edits. I hadn't touched the article since the 19th of November when you reverted to the 14th, so my edits that you removed had been stable for nearly the whole month and a half. You said, in your Jan 1st edit comment, "please redo any edits you think need to be redone"; I've said that I think they should all be, giving reasons, but asked you to please do the work. If you refuse, I'm offering to do the work, manually merging out of a reluctance to waste the efforts of intervening editors. Essentially, I'm counting your revert as the bold edit; I requested an unrevert here promptly, given the time of year. The article is still undergoing a major restructuring, and I don't think that helping with this is unfair, or disrespectful to Seppi333's efforts, but I will take recent changes into consideration. HLHJ (talk) 05:15, 10 February 2019 (UTC)
- The lede is no longer too long. Seppi333 made a lot of changes to the article. Going back to a previous version or merging a previous version will undo the edits by Seppi333. I counted your previous edits as bold edits that did not gain consensus. I told Seppi333 to redo his edits. Seppi333 did redo his edits. You are the only one objecting to the edits made by me and Seppi333. I'm not sure what you want to do. QuackGuru (talk) 12:56, 10 February 2019 (UTC)
- I agree that the lede is too long, but that's a side issue. I'm talking about a large revert including some of Seppi333's own edits. I hadn't touched the article since the 19th of November when you reverted to the 14th, so my edits that you removed had been stable for nearly the whole month and a half. You said, in your Jan 1st edit comment, "please redo any edits you think need to be redone"; I've said that I think they should all be, giving reasons, but asked you to please do the work. If you refuse, I'm offering to do the work, manually merging out of a reluctance to waste the efforts of intervening editors. Essentially, I'm counting your revert as the bold edit; I requested an unrevert here promptly, given the time of year. The article is still undergoing a major restructuring, and I don't think that helping with this is unfair, or disrespectful to Seppi333's efforts, but I will take recent changes into consideration. HLHJ (talk) 05:15, 10 February 2019 (UTC)
I'm not done with overhauling this article. I've just been too busy to edit Wikipedia this week. I'll probably continue sometime between Wednesday-Saturday. Seppi333 (Insert 2¢) 17:17, 10 February 2019 (UTC)
Cognitive harms in lede
Zvi Zig, you removed this statement from the lede:
The evidence suggests that exposure to nicotine between the ages of 10 and 25 years causes lasting harm to the brain and cognitive ability.[9] Nicotine use during pregnancy increases the child's risk of type 2 diabetes, obesity, hypertension, neurobehavioral defects, respiratory problems, and infertility.[10]
Your edit comments were "Violates WP:NPOV: The 2016 Royal College of Physicians' report "Nicoitne Without Smoke" (P. 59( doesn't deem evidence on this convincing" and "WP:NPOV violation: 2016 Royal College of Physicians' report "Nicoitne Without Smoke" (P. 59) doesn't deem evidence on this conclusive". I quote the report and page in question:
Research from animal studies suggests that fetal exposure to nicotine may lead to adverse postnatal health consequences and that cognitive function and development are adversely affected by nicotine exposure during both the fetal and the adolescent periods. The relevance of these findings to human brain development remains uncertain, however. There is evidence that smoking in adolescence is associated with cognitive and attentional impairments in later life, and possibly an increased risk of mental health problems, but it is difficult to exclude the effects of confounders of this association in the observational studies available.
This seems to be all that this report has to say on the topic. It does not seem to contradict the statement you removed from the article; it says that confounding factors are an issue in human observational studies, which was also discussed, much more throughly, in the SG report. This isn't surprising, as you cannot randomize 11-year-olds into two groups and tell half of them to take nicotine; your ethics committee would go through the roof at the suggestion. The Surgeon General's report is apparently somewhat more recent than the RCoP report, and is a much more through review, surveying and citing more literature and discussing it more extensively (there are nearly four pages on the mental effects of nicotine on young people, plus an appendix section). The SG report includes randomized animal trials as well as observational human trials and mechanistic arguments (see page 104 of the full report). The human trials use elaborate statistical techniques to derive results without using a randomized clinical trial; they search for and control for confounding factors, use paired twin studies, all the usual epidemiological workarounds. The Surgeon General's conclusions seem well-founded. May I ask that you restore this content? HLHJ (talk) 05:30, 13 January 2019 (UTC)
Sorry, I forgot to mention the fetal effects of maternal nicotine use. I didn't see anything in the report you cite suggesting that these fetal harms do not occur; have I missed something? HLHJ (talk) 02:19, 14 January 2019 (UTC)
- "The evidence suggests that exposure to nicotine between the ages of 10 and 25 years causes lasting harm to the brain and cognitive ability.[9]" This statement is too much detail for the lede. QuackGuru (talk) 15:13, 15 January 2019 (UTC)
- Thank you, HLHJ, for addressing my comment.
- The RCP report clearly concludes that no conclusion regarding nicotine and cognitive development effects can be made for humans. Even the Surgeon General's Report seems to imply the feebleness of its conclusion:
Limited direct human experimental data exist on the effects of nicotine exposure from e‑cigarettes on the developing adolescent brain, but experimental laboratory data have been found to be relevant in animal models to contextualize effects in humans.
- The RCP does not require randomized trials for causative inference (in fact it famously concluded smoking caused disease in 1962 based on observational studies alone[11]). However, it notes that "it is difficult to exclude the effects of confounders of this association in the observational studies available [emph. mine]".
- Furthermore, Surgeon General's conclusions on cognitive development have been subject to an extensive critique[12] and have not been included in the 2018 National Academy of Sciences comprehensive review on the public health consequences of e-cigarettes, which includes review of the effects of nicotine.[13].
- The twin study noted above also reports
Educational achievement did not differ within twin pairs discordant for smoking, in adults (p = .98) and adolescents (p = .49).[14]
- The twin study noted above also reports
- Also, Public Health England's 2018 evidence review concurs with RCP's uncertainty relating nicotine's adolescent and prenatal effects (p 60)[15]
- Therefore, I don't think that the Surgeon General's 2016 conclusion ends the debate.
- Zvi Zig (talk • contribs 08:27, 28 January 2019 (UTC)
- Working on reply... HLHJ (talk) 05:46, 31 January 2019 (UTC)
- The National Academy of Sciences review is regrettably behind a $100 US paywall. I have looked at its publicly-available conclusions, and you're right; they do not address the effects of nicotine in itself, possibly because the report is narrowly focussed on e-cigarettes.
- The extensive critique you cite, A critique of the US Surgeon General’s conclusions regarding e-cigarette use among youth and young adults in the United States of America, has substantial conflicts of interest, though I did not find this obvious at first glance. See, for instance, Tobacco Tactics on the lead author. Looking up the organizations in the COI statement gives similarly worrying results; "AEMSA" (named with just the unexpanded acronym, a bad sign) is the "American E-Liquid Manufacturing Standards Association". On close inspection, I cannot characterize this paper as an independent source, so I don't think it meets WP:RS.
- On to the British sources. In Britain, e-cigs are sold in pharmacies and are approved for smoking cessation, and I've heard claims that they are therefore more used by smokers and less by teens than is the case in the US. If so, this might explain why the British reports are far more interested in use by smokers, and less in use by non-smokers, than the US sources. You wrote:
The RCP report clearly concludes that no conclusion regarding nicotine and cognitive development effects can be made for humans.
- I quoted the paragraph from the RCP report in my first reply above. Epidemiologists make very fine a technical qualifications to conclusions, including levels of certainty. "No conclusion" would be reported as "No available evidence" or "Insufficient evidence" (to use the NAS terms), rather than "There is evidence that" or "Research in animals suggests". In my proposed text, I would like to exactly match the level of certainty given by the Surgeon General's report: "the evidence suggests". Utterly conclusive evidence is not needed to make such statement. Wikipedia does not need to re-do the metaanalysis, and can just report the conclusions of the most reliable and recent MEDRS; as the guideline puts it, we cite review, don't write them.
- I would not consider it inappropriate to discuss the types and limitations of the evidence behind this conclusion briefly in the article.
.jpg)
- The RCP report also says "It is possible that nicotine exposure during the fetal and/or adolescent periods causes cognitive impairment". This does not seem to me to contradict the Surgeon General's report. I should note that the RCP does not cite any sources on this issue except the 2014 Surgeon General's report (as the 2016 update wasn't out yet) and two reviews cited amongst other sources in the Surgeon General's report; that is to say, its evidence base is a proper subset of the evidence in the 2016 SG report.
Sources cited by the RCP review, with summaries, to illustrate scope
|
|---|
|
63: Bruin JE, Gerstein HC, AC Holloway. Long-term consequences of fetal and neonatal
nicotine exposure: a critical review. Toxicol Sci 2010;116:364–74. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2905398/ https://pdfs.semanticscholar.org/2da4/48399eec15249a754a5778185e179f3cd01f.pdf
64: US Department of Health and Human Services. The health consequences of smoking – 50 years of progress. A Report of the Surgeon General. Atlanta, GA: US Department of Health and Human Services, 2014. While this is obviously superceeded by the 2016 Surgeon General's report, it is interesting to note what it says:
65: Royal College of Physicians. Smoking and mental health. London: RCP, 2013. Totally irrelavent ot this point, as far as I can see; says that causality between smoking initiation and mentla health problems appears to run both ways. 66: Goriounova NA, Mansvelder HD. Short- and long-term consequences of nicotine exposure during adolescence for prefrontal cortex neuronal network function. Cold Spring Harb Perspect Med 2012;2:a012120. A highly technical review with little synthesis, it documents these harms well in human smokers and nicotine-dosed animals. As a side note, concluding that smoking causes disease in 1962 suggests a certain laggardliness, as pipe smoking had been connected to mouth cancers since the 1700s, there were reports of associations from the 1890s onwards, and the first solid epidemiological review on cigarettes came out in 1930. In German. Sadly, the war rather drowned it out, but everyone heard about the post-war results in 1951 when three simultaneous huge observational studies were published (one done on British doctors, which the RCP could hardly have missed). See History. |
- Public Health England's 2018 evidence review says:
A systematic review of nicotine was not carried out for this report because it was agreed by the commissioners that nicotine would have a stronger focus in a forthcoming PHE review. This chapter, therefore, briefly summarises and updates evidence in the Royal College of Physicians (RCP) report, focusing on nicotine addictiveness, nicotine delivery in relation to EC, and any recent evidence which suggested nicotine use could cause significant harm.
- They say that "The health effects of cleaner nicotine products per se is important, but the key comparison should be with smoking as, to our knowledge, no-one in public health is recommending nicotine to never smokers." This is true, but people outside public health recommend nicotine use to never-smokers all the time. Roachers are even paid to do it. Wikipedia has a more general audience, and I think should not contain only information that public health care providers need. The report also says that "These studies suggest that, for smokers, the [increased] risks of nicotine use are likely to be very low or negligible"; it does not assess the risk to non-smokers, though it states that people not using nicotine should not start.
Public Health England's 2018 evidence review
|
|---|
|
===== On nicotine use in pregnancy =====
Executive summary: "use of nicotine replacement therapy by pregnant smokers has not been found to increase risk to the foetus" (emphasis added) Body text: "There has been much concern about the use of EC by pregnant women and the role that nicotine may play in harming foetal development. Animal research has suggested foetal exposure to very high doses of nicotine has adverse consequences which are maintained through to adolescence, but the relevance for humans is unclear" This statement cites the following studies:
"In humans, it has been difficult to separate the impact of nicotine from smoking in pregnancy, given the low use of cleaner nicotine products among pregnant women. Thus assumptions about harms from nicotine in human pregnancies, have until recently, emerged either as a result of studies of tobacco use in pregnancy or are extrapolated from animal research. More recently, however, it has been reported that infants born to pregnant smokers, who used NRT for smoking cessation during pregnancy, were less likely to have developmental impairments compared with those who used placebo two years after birth" Citing:
"The reason for this requires more research but the authors argued it could be due to reduced smoking early in pregnancy as a consequence of NRT use. The licence for prescribing NRT was extended in the UK in 2005 to include use in pregnancy and NRT is currently widely prescribed in the UK to pregnant women who smoke", citing
"Limited research has been conducted with pregnant smokers or ex-smokers who use EC", citing
The section winds up by describing a study that is currently underway, and ends; that's the whole section. The paper doesn't address the question of whether the nicotine is harmful at all. They have only addressed the question of whether the children of smokers who tried to quit more during pregnancy (with NRT) are worse off than those who tried to quit less (without NRT). The cited study does suggest that nicotine from NRTs is less harmful than smoking, but that's also by-the-by. I really think they should have addressed the question of whether nicotine (from NRTs, to remove confounding factors such as other tobacco pyrolysis produts) is harmful compared to not using nicotine. I know that there are much better references on this, because I have added them to Wikipedia articles. I really thought I'd added them to this article, but they seem to have gone missing. Copied from another article:
On nicotine use in people of nicotine-addiction-acquisition age (11-25) |
- On the whole, the Surgeon General's report seems a better source for these statements.
- it directly addresses the statement at issue, namely the effects of nicotine consumption vs. non-consumption (not smoking vs. e-cig consumption).
- it reviews more sources, and more relevant sources
- it does a much more through job of going through the standard epidemiological methods of establishing causality in an area where RCTs are not ethical
- On the whole, the Surgeon General's report seems a better source for these statements.
Twin study
|
|---|
|
You're right, one of twin studies found no difference in educational attainment (which, since this is the Netherlands twin register, may mean "level of schooling completed", i.e. secondary, postsecondary; this is generally highly corellated with the parent's level of schooling). It found a difference in attentional deficits and the other factors.[25] But this is one individual primary source, and the sentence I added to the article did not make claims about educational attainment.
|
- I don't think you mentioned the effects of maternal nicotine in your reply; do you have any objection to having a sentence on that in the lede? HLHJ (talk) 21:58, 3 February 2019 (UTC)
- 1. I do think disagreements between US and UK reports in relation to the conclusiveness of evidence should be reflected.
- 2. The National Academies of Science report is available on their website for download by clicking "download ad guest" here[26].
- 3. Yes, that cited critique has COIs but is peer-reviewed. Not sure how that fits with WP:MEDRS but my point was only that there's no evidence the SGR ends the debate.
- 4. Ecigs are sold as a consumer products in UK https://www.gov.uk/guidance/e-cigarettes-regulations-for-consumer-products
- 5. The (2018) and RCP reports state uncertainty with regards to developmental cognitive effects in adolescents
smoking in adolescence has been associated with cognitive and attentional deficits and suggested to impact mental health, although confounding factors (such as self-selection) have not been taken into account thus far.
- This should be reflected (e.g. "research suggests that nicotine may... but more research is needed")
- 6. On fetal cognitive effects , the aforementioned PHE (p. 60) and RCP (p59) reports mention similar limitations. With regards to diabetes etc even the SGR mentions this as animal studies drawing no conclusions.
- Zvi Zig (talk • contribs 21:58, 8 February 2019 (UTC)
References
- ^ Cite error: The named reference
CancerResearch2013was invoked but never defined (see the help page). - ^ Cite error: The named reference
SGUS2014was invoked but never defined (see the help page). - ^ Cite error: The named reference
Parrott2015was invoked but never defined (see the help page). - ^ Parrott, Andrew C. (7 February 2006). "Nicotine psychobiology: how chronic-dose prospective studies can illuminate some of the theoretical issues from acute-dose research" (PDF). Psychopharmacology. 184 (3–4): 567–576. doi:10.1007/s00213-005-0294-y.
...nicotine dependency is a direct, albeit subtle, cause of psychobiological distress
- ^ Cite error: The named reference
Dependence-withdrawalwas invoked but never defined (see the help page). - ^ Cite error: The named reference
Parrott2003_normquotewas invoked but never defined (see the help page). - ^ Sajja RK, Rahman S, Cucullo L (March 2016). "Drugs of abuse and blood-brain barrier endothelial dysfunction: A focus on the role of oxidative stress". Journal of Cerebral Blood Flow and Metabolism. 36 (3): 539–54. doi:10.1177/0271678X15616978. PMC 4794105. PMID 26661236.
- ^ "The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General, 2014". www.surgeongeneral.gov.
There is insufficient data to conclude that nicotine causes or contributes to cancer in humans, but there is evidence showing possible oral, esophageal, or pancreatic cancer risks. Additionally, there is substantial experimental evidence indicating that nicotine is bioactive for a number of carcinogenic mechanisms in experimental systems. Although in vitro data are suggestive of relevant biological activity, this is not supported overall by the most recent experimental animal studies. In humans, there has been limited research and only one relatively short–term follow-up study [the 7-year Lung Health Study] on nicotine and cancer....The evidence is sufficient to infer that nicotine activates multiple biological pathways through which smoking increases risk for disease...The evidence is inadequate to infer the presence or absence of a causal relationship between exposure to nicotine and risk for cancer.
- ^ U.S. Department of Health and Human Services, Public Health Service Office of the Surgeon General Rockville, MD (2016). "E-Cigarette Use Among Youth and Young Adults: A Report of the Surgeon General". Retrieved 15 November 2018.
Evidence for this report was gathered from scientific research that included one or more of three age groups. These age groups included young adolescents (11–13 years of age), adolescents (14–17 years of age), and young adults (18–24 years of age). Some studies refer to the younger groups more generally as youth... Of concern with regard to current trends in e-cigarette use among youth and young adults, the evidence suggests that exposure to nicotine during this period of life may have lasting deleterious consequences for brain development, including detrimental effects on cognition
{{cite journal}}: Cite journal requires|journal=(help)CS1 maint: multiple names: authors list (link) - ^ Cite error: The named reference
Schraufnage2014was invoked but never defined (see the help page). - ^ https://www.rcplondon.ac.uk/projects/outputs/smoking-and-health-1962
- ^ https://harmreductionjournal.biomedcentral.com/articles/10.1186/s12954-017-0187-5?fref=gc&dti=802550153136903
- ^ https://www.nap.edu/catalog/24952/public-health-consequences-of-e-cigarettes
- ^ http://www.tweelingenregister.org/nederlands/verslaggeving/NTR-publicaties_2015/Treur_BP_2015.pdf
- ^ https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/684963/Evidence_review_of_e-cigarettes_and_heated_tobacco_products_2018.pdf
- ^ "Electronic Cigarettes – What are the health effects of using e-cigarettes?" (PDF). Centers for Disease Control and Prevention. 22 February 2018.
- ^ Slotkin, TA (June 1998). "Fetal nicotine or cocaine exposure: which one is worse?". The Journal of pharmacology and experimental therapeutics. 285 (3): 931–45. PMID 9618392.
- ^ Slotkin, TA; Lappi, SE; McCook, EC; Lorber, BA; Seidler, FJ (1995). "Loss of neonatal hypoxia tolerance after prenatal nicotine exposure: implications for sudden infant death syndrome". Brain research bulletin. 38 (1): 69–75. PMID 7552377.
- ^ Cooper, S; Taggar, J; Lewis, S; Marlow, N; Dickinson, A; Whitemore, R; Coleman, T; Smoking, Nicotine and Pregnancy (SNAP) Trial, Team. (September 2014). "Effect of nicotine patches in pregnancy on infant and maternal outcomes at 2 years: follow-up from the randomised, double-blind, placebo-controlled SNAP trial". The Lancet. Respiratory medicine. 2 (9): 728–37. doi:10.1016/S2213-2600(14)70157-2. PMID 25127405.
- ^ Brose, Leonie S.; McEwen, Andy; West, Robert (October 2013). "Association between nicotine replacement therapy use in pregnancy and smoking cessation". Drug and Alcohol Dependence. 132 (3): 660–664. doi:10.1016/j.drugalcdep.2013.04.017.
- ^ Oncken, Cheryl; Ricci, Karen A.; Kuo, Chia-Ling; Dornelas, Ellen; Kranzler, Henry R.; Sankey, Heather Z. (May 2017). "Correlates of Electronic Cigarettes Use Before and During Pregnancy". Nicotine & Tobacco Research. 19 (5): 585–590. doi:10.1093/ntr/ntw225.
- ^ Bruin, Jennifer E.; Gerstein, Hertzel C.; Holloway, Alison C. (2 April 2010). "Long-Term Consequences of Fetal and Neonatal Nicotine Exposure: A Critical Review". Toxicological Sciences. 116 (2): 364–374. doi:10.1093/toxsci/kfq103. ISSN 1096-6080. PMC 2905398. PMID 20363831.
Overall, the evidence provided in this review overwhelmingly indicates that nicotine should no longer be considered the safe component of cigarette smoke. In fact, many of the adverse postnatal health outcomes associated with maternal smoking during pregnancy may be attributable, at least in part, to nicotine alone.
- ^ England, Lucinda J.; Kim, Shin Y.; Tomar, Scott L.; Ray, Cecily S.; Gupta, Prakash C.; Eissenberg, Thomas; Cnattingius, Sven; Bernert, John T.; Tita, Alan Thevenet N.; Winn, Deborah M.; Djordjevic, Mirjana V.; Lambe, Mats; Stamilio, David; Chipato, Tsungai; Tolosa, Jorge E. (31 December 2010). "Non-cigarette tobacco use among women and adverse pregnancy outcomes". Acta Obstetricia et Gynecologica Scandinavica. 89 (4): 454–464. doi:10.3109/00016341003605719. ISSN 1600-0412. PMC 5881107. PMID 20225987.
The use of any products containing nicotine likely will have adverse effects of fetal neurological development.
- ^ Schraufnagel DE, Blasi F, Drummond MB, Lam DC, Latif E, Rosen MJ, Sansores R, Van Zyl-Smit R (September 2014). "Electronic cigarettes. A position statement of the forum of international respiratory societies" (PDF). American Journal of Respiratory and Critical Care Medicine. 190 (6): 611–8. doi:10.1164/rccm.201407-1198PP. PMID 25006874.
- ^ Treur, Jorien L.; Willemsen, Gonneke; Bartels, Meike; Geels, Lot M.; van Beek, Jenny H.D.A.; Huppertz, Charlotte; van Beijsterveldt, Catharina E.M.; Boomsma, Dorret I.; Vink, Jacqueline M. (November 2015). "Smoking During Adolescence as a Risk Factor for Attention Problems" (PDF). Biological Psychiatry. 78 (9): 656–663. doi:10.1016/j.biopsych.2014.06.019.
- ^ https://www.nap.edu/login.php?record_id=24952
- The UK reports discuss harms of nicotine to smokers; essentially, if smokers switch to another nicotine source, they are unlikely to be at additional risk from nicotine. I don't think the US reports disagree with their statements on that. So I've rephrased the article like this: "Nicotine use as a tool for quitting smoking has a good safety history.[26] The general medical position is that nicotine itself poses few additional health risks to smokers.[27] However, nicotine is harmful to non-users,[28] and research suggests that it harms brain development[28] in people in their mid-twenties and younger.[29][28]" There are much better sources on the fetal effects of nicotine, so I'll deal with that separately. HLHJ (talk) 00:36, 19 May 2019 (UTC)
New content
I do not review the new content and recent changes. I usually review the new content. I don't have the time. I wanted to let others know I am not following the changes. QuackGuru (talk) 20:06, 11 January 2019 (UTC)
- I deleted all of the article text that was added in those edits. Seppi333 (Insert 2¢) 18:05, 27 January 2019 (UTC)
- Why did you delete all of my edits? User109012 (Talk) 22:04, 28 January 2019 (UTC)
- WP:MEDANIMAL. Seppi333 (Insert 2¢) 02:59, 29 January 2019 (UTC)
- To be fair, when I first started editing, I added primary sources to drug articles like you did. Virtually all of my edits were reverted at the time, so I understand where you're coming from. You need to read WP:MEDRS in order to understand what kind of sources are acceptable to cite and what kind of information is appropriate to cover in a Wikipedia article (specifically, as it pertains to animal studies, which is covered in WP:MEDANIMAL). To give you a quick summary (NB: you still need to read WP:MEDRS), if you're citing a peer-reviewed journal article, it needs to be published recently (typically, within the past 5-10 years), be listed as a "Review", "Systematic review", or "Meta-analysis" under the "Publication types" tab on Pubmed, and it needs to cover clinical studies in humans, not just in vitro and animal studies. Seppi333 (Insert 2¢) 15:59, 29 January 2019 (UTC)
- I already responded to you further down but I'll copy it here. My edits are very on-topic, precise, current about research about a chemical, NOT a drug, and its effects on biological systems, not humans. This follows your change of a template of this article to a infodrug template, but it clearly states that this is an article about a chemical. It has nothing to do with MEDRS. For clarity, I add Research non-health related section but the information is specific to nicotine and utmost pertinent to the topic. User109012 (Talk) 18:08, 28 January 2019 (UTC)
- This is not a drug article. It's an article about a chemical, as stated at the top of the page. This article is missing an MSDS link for nicotine, which exists because it's a chemical, but you've changed this template to Infodrug template, so I don't know where to add that.User109012 (Talk) 18:13, 28 January 2019 (UTC)
- @User109012: regardless of whether the text is nominally about the chemical aspects (e.g., a fire diamond), the pharmacological aspects, the clinical aspects, or any other facet of a topic about a compound, if you write a biomedical claim, WP:MEDRS applies to the statement. If you want to add something to this article about what you've written, replace the primary sources (PMID 28398760, 25668718, 24687640, 29066952) with secondary ones and do not misleadingly suggest that in vitro research applies to humans (e.g., how you wrote about PMID 28398760) again. This is the last time I'm going to say this before I bring this issue to the attention of admins. Read WP:Edit warring. Seppi333 (Insert 2¢) 19:16, 29 January 2019 (UTC)
- @Seppi333: There is something very shady in claiming research on purely biomolecular effects of a high-sales chemical in non-clinical settings on non-human organisms is biomedical and blocking information on that ground. Scientists do molecular research using chemicals and that has nothing to do with clinical trials and humans. Without that research in this Wiki article about a chemical molecular cell biologists or students will not be informed about usability of this chemical in biology labs and educate themselves for future research ideas to benefit humanity. Is that what you are trying to accomplish? User109012 (Talk) 05:21, 30 January 2019 (UTC)
- Hmm. Well, I've only been editing medical articles on a more-or-less daily basis for about 6 years or so; but, I'll entertain your idea that I might not understand a policy that new editors (even me, way back when) tend to find themselves at odds with when editing articles on a biologically active compound like this one. So, I've asked others at Wikipedia Talk:WikiProject Medicine to weigh in on whether or not WP:MEDRS applies to these statements that you added. Seppi333 (Insert 2¢) 06:30, 30 January 2019 (UTC)
- @Seppi333: There is something very shady in claiming research on purely biomolecular effects of a high-sales chemical in non-clinical settings on non-human organisms is biomedical and blocking information on that ground. Scientists do molecular research using chemicals and that has nothing to do with clinical trials and humans. Without that research in this Wiki article about a chemical molecular cell biologists or students will not be informed about usability of this chemical in biology labs and educate themselves for future research ideas to benefit humanity. Is that what you are trying to accomplish? User109012 (Talk) 05:21, 30 January 2019 (UTC)
- As for the MSDS, add that to the external links section. Seppi333 (Insert 2¢) 19:21, 29 January 2019 (UTC)
- @User109012: regardless of whether the text is nominally about the chemical aspects (e.g., a fire diamond), the pharmacological aspects, the clinical aspects, or any other facet of a topic about a compound, if you write a biomedical claim, WP:MEDRS applies to the statement. If you want to add something to this article about what you've written, replace the primary sources (PMID 28398760, 25668718, 24687640, 29066952) with secondary ones and do not misleadingly suggest that in vitro research applies to humans (e.g., how you wrote about PMID 28398760) again. This is the last time I'm going to say this before I bring this issue to the attention of admins. Read WP:Edit warring. Seppi333 (Insert 2¢) 19:16, 29 January 2019 (UTC)
I've added PubChem's safety data sheet to the external links section. Seppi333 (Insert 2¢) 01:11, 16 February 2019 (UTC)
@WikiProject Medicine
Do all of these statements[note 1] fall within the purview of WP:MEDRS, or are some of these not biomedical claims? Seppi333 (Insert 2¢) 06:30, 30 January 2019 (UTC)
- My two cents: I cannot see how a zebrafish assertion would fall under MEDRS. The immune section, if the article is about macrophages and human immunity, probably MEDRS. The human sleep assertion does seem to fall under MEDRS--human sleep is definitely a medical/health issue. The mouse sleep assertion would not, but I think the prose needs to make clear that this is an assertion about mice, not humans. --
{{u|Mark viking}} {Talk}07:51, 30 January 2019 (UTC)- @Mark viking: if that’s your take on this, then, in your opinion, when would WP:MEDANIMAL ever apply to drug article statements and the corresponding source? Seppi333 (Insert 2¢) 11:01, 30 January 2019 (UTC)
- Thanks for your thoughtful question. I think MEDANIMAL does apply in these passages. Animal experiments don't generate direct human clinical implications, and so as that guideline says, the prose should make clear that these are animal experimental results that are being cited. with no direct human implications. But this might reflect my bias--in clinical human genetics, animal expts can be suggestive, but should not be used as direct evidence in a clinical diagnosis. Perhaps the animal-human link is considered more direct in pharmacology? If so, then MEDANIMAL should become more context dependent, based on the kind of experiment, and my opinions above are less relevant. --
{{u|Mark viking}} {Talk}19:00, 30 January 2019 (UTC)
- Thanks for your thoughtful question. I think MEDANIMAL does apply in these passages. Animal experiments don't generate direct human clinical implications, and so as that guideline says, the prose should make clear that these are animal experimental results that are being cited. with no direct human implications. But this might reflect my bias--in clinical human genetics, animal expts can be suggestive, but should not be used as direct evidence in a clinical diagnosis. Perhaps the animal-human link is considered more direct in pharmacology? If so, then MEDANIMAL should become more context dependent, based on the kind of experiment, and my opinions above are less relevant. --
- @Mark viking: if that’s your take on this, then, in your opinion, when would WP:MEDANIMAL ever apply to drug article statements and the corresponding source? Seppi333 (Insert 2¢) 11:01, 30 January 2019 (UTC)
- What does "fall within the purview of MEDRS" mean to you? In recent years, this phrase usually is associated with a desire to blank anything that isn't followed by a source that does not meet MEDRS's "ideal" qualities.
- I think it might be more relevant to consider whether this content is WP:DUE. For example, the claim that nicotine disrupts sleep: that's probably encyclopedia information that ought to be included, ideally with the best source you can find. But the claim that the mechanism for that disruption is some particular pathway? Hmm, that's not so obviously relevant to a general article, but it would likely be appropriate to mention in an article about the physiology of nicotine. If editors happened to agree with my assessment of the importance of that particular detail (which they might not, and that's okay with me), then it doesn't matter if it "falls within the purview of WP:MEDRS", because it doesn't belong in the article at all. WhatamIdoing (talk) 16:39, 30 January 2019 (UTC)
What does "fall within the purview of MEDRS" mean to you?
- it means that the corresponding statement in the article text is a biomedical claim. My interpretation of MEDANIMAL is very straightforward: if something is stated about an animal and the equivalent statement about humans is clinically relevant, then it's a medical claim that, per that section of MEDRS, requires a secondary source. The study about developmental toxicity in zebrafish is an animal model for developmental toxicity in humans. The study about knockout mice is an animal model for the molecular mechanisms underlying sleep perturbations by nicotine in humans. And then there's PMID 28398760; the issue with that source should not require an explanation. But, if everyone comes to the consensus that dumping primary animal research and primary in vitro research into topically-relevant (sub)-articles is perfectly fine, I'll revert all my edits to this article and restore the garbage heap that it was previously; I deleted a lot of in vitro and animal research that shouldn't go to waste.- Re:
the claim that nicotine disrupts sleep: that's probably encyclopedia information that ought to be included, ideally with the best source you can find.
When I deleted it the first time around, I replaced it with this. - Re:
this phrase usually is associated with a desire to blank anything that isn't followed by a source that does not meet MEDRS's "ideal" qualities.
that's the only way to handle cherry picking; the point of a citing a review is to provide context to the evidence from primary research, which could be grossly misleading when it's not reproducible or is at odds with other lines of evidence. Seppi333 (Insert 2¢) 17:46, 30 January 2019 (UTC)- In the case of cherry-picking, you might be correct. In the case of someone citing a primary source because that's normal for academics, and they didn't realize that Wikipedia doesn't care about scientific priority, then blanking is the wrong response, and replacing (or supplementing) the primary source with a higher quality source is the correct response. WhatamIdoing (talk) 17:01, 6 February 2019 (UTC)
- WP:RS also says use high quality secondary sources. So Would trim the content based on primary sources. Doc James (talk · contribs · email) 01:37, 31 January 2019 (UTC)
- agree w/ Doc James--Ozzie10aaaa (talk) 11:40, 31 January 2019 (UTC)
- MEDRS applies to the content in the diff above. There are numerous reviews on this topic. I would remove the primary medical sources. QuackGuru (talk) 23:00, 31 January 2019 (UTC)
References
- ^ except for the first sentence under the Immune system heading ("
Immune cells of both innate and acquired immune subsystems frequently express the α2, α5, α6, α7, α9, and α10 subunits of nicotinic acetylcholine receptors.
"), which IMO falls within the scope of WP:SCIRS. It happens to be cited by a medical review anyway, so I don't have an issue with it.
WP:MEDANIMAL, adverse effects of tobacco exposure, and drug monographs
I intend to delete the vast majority of content discussing in vitro and animal research in this article; the only exception is content cited to a review which makes a statement about humans on the basis of animal research. In general, if you can't make a statement about humans because reviews don't say anything about it, don't look for preclinical sources.
Also, the vast majority of the adverse effects section cites sources about smoking and tobacco... yet again. This article is not about tobacco, but most of this section is a WP:COATRACK about tobacco. All of that needs to be replaced with statements about clinical effects/human exposure from drug monographs, which I know I've suggested before. These are drug monographs on nicotine:
- IPCS: http://www.inchem.org/documents/pims/chemical/nicotine.htm
- ECHA: https://echa.europa.eu/documents/10162/31694def-b7c3-208d-5aaf-3db9681ec3b9
- TOXNET: http://toxnet.nlm.nih.gov/cgi-bin/sis/search2/r?dbs+hsdb:@term+@DOCNO+1107
I'll do that at some point in the future. Seppi333 (Insert 2¢) 13:12, 23 January 2019 (UTC)
- This article's adverse effects section really is a nightmare. There isn't a single adverse effect covered, there's tons of random crap about tobacco/smoking, there's a number of primary sources, and sections like the one on immune function overstate what's written in the sources. The first source on nAchRs states that the receptors themselves are involved in immune regulation; that means all receptor ligands influence it, not nicotine alone. The second primary source states that nicotine influences a single bacterial infection, but the article says "... impair macrophage killing of deadly global human pathogenic bacteria". Just WTF is going on here? I'm going to delete massive swaths of text like this right now. Seppi333 (Insert 2¢) 16:11, 23 January 2019 (UTC)
- Ok. After cutting an excessive amount of redundant, off-topic, excessively vague, and primary-sourced content, Special:Permalink/879876010 is what we have left. If at some point this article ends up as a mass of statements like the ones I had to cut out, I intend to revert it back to this permalinked revision and restore any useful subsequent additions. The adverse effects and overdose sections are supposed to include the drug's side effects and overdose symptoms, so that's what I'm going to put there when I expand those sections. Seppi333 (Insert 2¢) 18:14, 23 January 2019 (UTC)
- You delete my edits that are very on-topic, precise, current about research about a chemical, NOT a drug, and its effects on biological systems, not humans. This follows your change of a template of this article to a infodrug template, but it clearly states that this is an article about a chemical. For clarity, I can add Research non-health related section but the information is specific to nicotine and utmost pertinent to the topic. User109012 (Talk) 17:32, 29 January 2019 (UTC)
- If there's an issue with a single bacterial infection vs an infection by a deadly global human pathogenic bacteria, that can be improved, but not "WTF"'d into obsoletion by Seppi333. User109012 (Talk) 17:42, 29 January 2019 (UTC)
- You delete my edits that are very on-topic, precise, current about research about a chemical, NOT a drug, and its effects on biological systems, not humans. This follows your change of a template of this article to a infodrug template, but it clearly states that this is an article about a chemical. For clarity, I can add Research non-health related section but the information is specific to nicotine and utmost pertinent to the topic. User109012 (Talk) 17:32, 29 January 2019 (UTC)
- Ok. After cutting an excessive amount of redundant, off-topic, excessively vague, and primary-sourced content, Special:Permalink/879876010 is what we have left. If at some point this article ends up as a mass of statements like the ones I had to cut out, I intend to revert it back to this permalinked revision and restore any useful subsequent additions. The adverse effects and overdose sections are supposed to include the drug's side effects and overdose symptoms, so that's what I'm going to put there when I expand those sections. Seppi333 (Insert 2¢) 18:14, 23 January 2019 (UTC)
Content from paywalled sleep review
Nicotine
Studies examining the effect of acute nicotine intoxication on sleep using transdermal nicotine application in nonsmokers reported a dose-dependent reduction of REM sleep, slow wave sleep, and total sleep time.12,13 During acute intoxication, nicotine, similar to other stimulants, increases REM latency, sleep onset latency, and NREM 2 sleep.13
Chronic smokers were reported to have twice the risk of experiencing sleep disturbances, the most common including increased sleep latency and daytime sleepiness.12 Nicotine consumption in chronic smokers was also linked to decreased total sleep time and increased REM latency. When compared to non-smokers, chronic smokers had a decreased slow wave sleep (SWS) and reduced sleep efficiency.12
Nicotine withdrawal, following cessation of nicotine administration in non-smokers, was associated with increased total sleep time and REM rebound (a phenomenon in which increased frequency and length of REM sleep occurs) on PSG studies.12,13 The effects of withdrawal on sleep are dose dependent, but usually begin 6–12 hours after cessation of nicotine, reach a maximum within 1–3 days, and can continue for up to 3 weeks.12 Effects include an increase in REM sleep and wake after sleep onset, and decrease in REM latency and sleep onset latency.12,13 Subjective measurements depict a decrease in sleep quality and increased depressive symptoms.13
— PMID 26346395
Changes to Fetal development and breastfeeding
Seppi333 did an excellent job of tightening the section and removing meaningless content. The entire section was rewritten. Let try to work toward consensus with all involved editors. @Seppi333: do you have time to review the changes? QuackGuru (talk) 22:28, 3 February 2019 (UTC)
- I'll return to this article sometime this week. Seppi333 (Insert 2¢) 21:54, 10 February 2019 (UTC)
- I should have time to start working on this article again later today or sometime tomorrow. Seppi333 (Insert 2¢) 00:24, 16 February 2019 (UTC)
I will eventually - likely within the next month or two - get around to finishing the expansion of this article; I've been preoccupied with other things lately, so I haven't really had the time/energy for content creation on the scale that this article requires right now. If anyone else is interested in doing this, feel free to expand the sections I've marked. The sources I listed in the maintenance tags are the most recent topically-focused reviews on those subtopics that I found on Pubmed. Seppi333 (Insert 2¢) 20:59, 10 March 2019 (UTC)
No medical use of nicotine
The page erroneously implies that there are medical uses of nicotine. There are none. There is limited medical use of nicotine delivery vehicles such as patches, lozenges, sprays, but not of the chemical itself. The 2016 rerort by the Royal College of Physicians cited on the page refers to the long-term substitution of nicotine source as the medical recommendation, not to the presence of nicotine specifically in treatment. On opposite - they recommend substitution of source only as the second best alternative to complete discontinuation of all nicotine use. In other words, they indirectly endorse recreational - not medical - use of nicotine from, as they write, "less hazardous nicotine source." And it is largely common sense, too. We don't give radiation treatments to patients with radiation sickness. Or we don't prescribe more oxygen deprivation to people who are already suffocating or oxygen deprived. Or we don't administer more poison to people who are dying from intoxication by that same poison - we give antidotes. We endorse medical use of devices and/or approaches for "harm reduction" (also a major focus of the Royal College of Physicians report) to minimize harm and wean people off of highly addictive substances. No source in the Medical Use section states there are medical uses of this substance. The page should clearly state that there are no medical (or therapeutic) uses for nicotine. @Seppi333: User109012 (Talk) 08:15, 15 February 2019 (UTC)
- @User109012: Nicotine is the active ingredient in around 1–2 dozen FDA-approved drug products; you can easily verify this by following this link, entering "nicotine" into the search field, pressing enter, and expanding the all of the entries in the search results.
- Also, based upon what you've written above, you seem to be confusing a dosage form with an active ingredient. A dosage form simply serves as a delivery vehicle for an active ingredient via a specific route of administration. Dosage forms contain one or more active ingredient(s) and almost always contain excipients (i.e., "other stuff", like the binding agents in a nicotine lozenge: nicotine polacrilex is the active ingredient in the lozenge, where nicotine is the [pharmacologically] active moiety and Poly(methacrylic acid) is the inactive moiety in nicotine polacrilex) unless the active ingredient can be given in a pure form without the need for an excipient via a specific route (e.g., intravenously via an IV drip line or hypodermic needle, but even then, a medication is often diluted in saline when given via this route). Seppi333 (Insert 2¢) 00:24, 16 February 2019 (UTC)
- @Seppi333: Yes, FDA refers to those products as "medicinal nicotine products," not drugs: [4]. If you saw "drug" in the FDA search of approved drugs link you sent, it may be due to limitations of their search engine database, and IT is not a good authority on this matter.
- FDA also lumps safety and regulation of tobacco products together with nicotine, they do not place it under their drug regulation mission (see top of page): [5]. Nicotine then, according to FDA, is not a medical drug with medical use, it's an ingredient of "a medicinal product." The medicinal property of those medicinal products is not in nicotine being an ingredient, but in the change of its route of administration, which is, what medical professionals agree on, the harm reduction therapy, as clearly seen in the Royal College of Medicine report.
- Dosage form is relevant only in the context of inactive moeities' function of stabilization and delivery being part of the alternative route of administration that's medicinal. User109012 (Talk) 11:49, 16 February 2019 (UTC)
- @Seppi333:To exhaustively prove that nicotine has no medical uses - Nicotine Material Safety Data Sheet does not have "pharmaceutical product used for smoking cessation" listed in identified uses, unlike the drug varenicline for reference, which does. MSDS is not prominently linked on this page as it is for other chemicals, and when I suggested to include that you suggested to include it in External Links. It helps to clear these things up. User109012 (Talk) 15:15, 16 February 2019 (UTC)
- Isn't the nicotine inhaler still a prescription-only product in US? Nicotine is the only active ingredient and it's a medical prescription, so it seems like that is exactly a "medical use". That ref intro is "NICOTROL NS (nicotine nasal spray) is indicated as an aid to smoking cessation for the relief of nicotine withdrawal symptoms." "For the relief of...symptoms" is exactly a medical claim. DMacks (talk) 16:46, 16 February 2019 (UTC)
- @DMacks: Nicotine in tobacco cigarettes also relieves nicotine withdrawal symptoms in smokers, which is at the essence of this very harmful addiction. Smoking for the relief of nicotine withdrawal symptoms is hardly a medical claim. Just as it is not a medical claim with nicotine nasal sprays. Medical professionals try to stop people from all nicotine use, not endorse more of it. They do it via endorsement of alternative sources of nicotine, not nicotine itself. This has been already stated on this page. User109012 (Talk) 11:20, 18 February 2019 (UTC)
Medical professionals try to stop people from all nicotine use, not endorse more of it.
Corrected version: Medical professionals try to stop people from all
Seppi333 (Insert 2¢) 15:38, 18 February 2019 (UTC)
nicotine tobacco use, not endorse more of it.
|
How to find MEDRS-compliant sources
@User109012: Since I didn't really offer any guidance on how to search PubMed for WP:MEDRS-compliant sources earlier, I figured I should give you some guidance on how to do this now.
If you follow this link and replace the "( ENTER_YOUR_SEARCH_TERMS_HERE )
" text in the search bar with a search string – like ("Nicotine"[Title/abstract] AND "Sleep"[Title/abstract])
(link to this search) or even just (Nicotine sleep)
(link to this search) – then every source that shows up in your search results will be a MEDRS-compliant source that you can use to cite medical claims in this article.
This is because the additional search constraints that I included in that link (i.e., the "AND ((Review[ptyp] OR systematic[sb] OR Meta-Analysis[ptyp]) AND "2009/02/18"[PDat] : "2019/02/15"[PDat])
" text that appears in the search bar) limits all of the search results to reviews, systematic reviews, and meta-analyses which were published within the past 10 years; those 3 types of sources are MEDRS-compliant and the 10 year window is reasonably acceptable for satisfying WP:MEDDATE. Seppi333 (Insert 2¢) 00:42, 16 February 2019 (UTC)
No MSDS hazard info displayed on a highly toxic chemical & no chemical properties table
Nicotine is a highly toxic chemical but chemical lab users coming to this Wiki page don't get prominent hazard and safety warnings from MSDS, unlike on other pages for chemicals. And we are supposed to debate about this? When I suggested to include MSDS info you suggested to link it in External Links.
The template for this page should also have chemical properties summary table as it is used in chemical laboratories for chemical synthesis. It doesn't have it right now, unlike other pages for chemicals. @Seppi333: User109012 (Talk) 15:29, 16 February 2019 (UTC)
- This article is written as a "drug" article not a "chemical" article, so it has a {{Infobox drug}} not {{chembox}} as the summary at the top–right of the article. Individual articles can only use the fields that each of those templates supplies, they cannot arbitrarily decide to add other ones. The chem case is all sorts of details about the chemical whereas the drug case is more tightly focused on pharmaceutical details. I think it will be difficult to get consensus to change this article to be "chemical" instead of "drug". So instead you might want to check with the infobox-drug centralized template and see if they would be willing to support an SDS (it's not called "MSDS" any more:) or other hazard detail. DMacks (talk) 16:38, 16 February 2019 (UTC)
- @DMacks: Why do you believe that it will be difficult to get consensus to change this article about a chemical to be "chemical" instead of "drug" when there are safety warnings missing in the article? Just a link to SDS is not going to help chemists and the public to be aware of the acute toxicity to humans and toxicty to aquatic life of chemical nicotine. Nicotine is FATAL if swallowed or in contact with skin! @Seppi333:User109012 (Talk) 11:33, 18 February 2019 (UTC)
- Nicotine is nowhere near as toxic as some monographs suggest. ER visits due to (non-fatal) nicotine poisoning that involved much higher doses than the purported lethal dose have been reported. See [6] sections "4.2.1.4 Acute toxicity: other routes"/"4.2.2 Human information". Honestly, I'd be inclined to delete SDS data on toxicology if it were included in an article because those monographs are intended to communicate potential chemical hazards, not toxicology information; instead, toxicology monographs should be sourced for content on that. Seppi333 (Insert 2¢) 13:51, 18 February 2019 (UTC)
- @DMacks: Why do you believe that it will be difficult to get consensus to change this article about a chemical to be "chemical" instead of "drug" when there are safety warnings missing in the article? Just a link to SDS is not going to help chemists and the public to be aware of the acute toxicity to humans and toxicty to aquatic life of chemical nicotine. Nicotine is FATAL if swallowed or in contact with skin! @Seppi333:User109012 (Talk) 11:33, 18 February 2019 (UTC)
Photoactivatable Nicotine
First, I want to claim that I'm not a frequent editor/contributor to wikipedia (but i do donate).
I saw that the nicotine page was under construction and I felt it may be relevant to add a section addressing a new scientific tool (https://www.nature.com/articles/nmeth.4637). Full disclosure, I am an author on that publication. — Preceding unsigned comment added by Cicatrix768 (talk • contribs) 21:15, 14 March 2019 (UTC)
- Normally I'd want to cite a secondary source, but since that paper just discusses a pharmacology research tool and since the paper has been cited by at least 2 other studies which utilized it, I went ahead and cited the source you provided here. Seppi333 (Insert 2¢) 13:57, 11 April 2019 (UTC)
Sourced content replaced with failed verification content
This edit restored failed verification content. QuackGuru (talk) 15:58, 26 March 2019 (UTC)
- The linked pages spoke for themselves, and the original summary was antiquated and lacking a true summarization of nicotine's uses and recognition to most people. The content verified themselves — if anyone would've clicked into any of the four linked pages, they all backed up exactly what was stated. ± AlBashir (talk 04:46, 27 March 2019 (UTC)
- That is not a summary. For example, this article is not about e-cigs. These edits violated summary. QuackGuru (talk) 17:14, 27 March 2019 (UTC)
- Please understand that saying "Nicotine is the primary active ingreedient in Tobacco, e-cigs, etc.. & named after Jean Nicot." is a much better summary than "Nicotine use disorders". — Preceding unsigned comment added by AlBashir (talk • contribs) 23:01, 27 March 2019 (UTC)
This change greatly improved the lede. A better summary has been restored without the failed verification content. QuackGuru (talk) 20:48, 27 March 2019 (UTC)
- The current lead is how the lead of a drug article is written. It follows MOS:PHARM. The reverted revision is not an improvement. Seppi333 (Insert 2¢) 23:31, 27 March 2019 (UTC)
- I'll conceed that the mention of Nicot is not how it is usually done, and I apologize for that. But the uses I edited in are definetely in-line with leads of other drugs, please see Caffeine as it is the most relevant example. Nicotine does not quite help with "Nicotine use disorder", that is like saying Heroine is the aid for "Opiate Use Disorder". — Preceding unsigned comment added by AlBashir (talk • contribs) 23:37, 27 March 2019 (UTC)
- Nicotine (as in, nicotine replacement therapy) is used as a treatment for nicotine dependence in nicotine-dependent individual, including both those who intend to wean off and those who are unwilling to quit entirely. While the latter is not an ideal solution since it entails lifelong nicotine use, it is an approved medical use in either case. FWIW, the analogy of nicotine with heroin would actually be using opioid replacement therapy for heroin addiction/dependence. Seppi333 (Insert 2¢) 14:06, 11 April 2019 (UTC)
- Also, as an afterthought, the DSM-5 calls it “tobacco use disorder”. Seppi333 (Insert 2¢) 14:40, 11 April 2019 (UTC)
Cigarette nicotine yield
Para 3 of the lede states "An average cigarette yields about 2 mg of absorbed nicotine". While this is in the ref cited (Mayer B January 2014), it is mentioned rather casually in passing without a citation. If memory serves, I have often seen figures of 1-1.2 mg delivered per cigarette. Also, if I remember correctly, the article at one time gave a figure closer to 1 mg.
In any case, the absorbed dose must depend on the size of cigarette, type of tobacco, etc., and may change (almost certainly has changed) over time; moreover, actual figures for yield/absorbed dose do not appear in the body of the article, so I don't think this belongs in the lede. As this is a much-edited and highly notable article, I don't want to just jump in & arbitrarily change it without input from other editors. Also, I haven't so far found good sources for nicotine yield, though there must be plenty out there. So——
- Does this belong in the lede?
- Is the figure correct in broad terms?
- Does anyone have some really authoritative sources, e.g. surgeon-general, govt. labs etc?
--D Anthony Patriarche (talk) 14:04, 29 March 2019 (UTC)
- I have no opinion as to whether it should go into the lead. I have no clue if that statement is factually accurate; although, I do remember reading in a source somewhere that nicotine yields vary by brand. There's got to be something from the surgeon general on that though. Seppi333 (Insert 2¢) 14:00, 11 April 2019 (UTC)
- "The average cigarette contains 10–15 mg of nicotine and delivers, on average, roughly 1–2 mg of nicotine systemically to the smoker."
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4958544/
- Zvi Zig (talk • contribs 23:12, 17 April 2019 (UTC)
- I have no opinion as to whether it should go into the lead. I have no clue if that statement is factually accurate; although, I do remember reading in a source somewhere that nicotine yields vary by brand. There's got to be something from the surgeon general on that though. Seppi333 (Insert 2¢) 14:00, 11 April 2019 (UTC)
Little information on positive effects of nicotine
Nicotine must have some good effects as it's been used by millions for centuries. The introduction section is essentially a long list of the dangers of the drug, and use of the drug is only discussed in the context of gradually quitting to avoid hard onset of withdrawal symptoms. I think it may make sense to place more emphasis on the actual reason the drug is widely used, and not merely to assume that the only interesting information would pertain to potential dangers. Let me know what you think. RF 67.166.141.33 (talk) 05:57, 12 May 2019 (UTC) RF
- Until recently, all nicotine use for centuries has been limited to tobacco use. And technically, the foremost reasons it’s widely used (as part of tobacco) is the 2 diseases mentioned in the lead (addiction/dependence) for which pure nicotine is used as a medical treatment. Seppi333 (Insert 2¢) 08:06, 12 May 2019 (UTC)
- I would argue the foremost reason it has been used extensively is rather the effects it has once it's been processed pharmacologically by the body. People didn't use cigarettes as currency in POW camps because they wanted to stop their addiction, they did it because cigarettes make people feel good, (so they were actually using it to continue their addiction.) This is what makes it appealing and thus addicting and widespread. An introduction should include the most basic, essential points about a subject. This seems to me to be an essential piece of information because it's the whole reason the molecule is of interest in the first place. The lack of any mention of the reason nicotine has appeal to people contrasted with extensive reference to risks makes the introduction read a little like anti-drug propaganda. Just stating that it's a "potent parasympathomimetic alkaloid" is not very useful for most people who want to understand the reason people inhale tobacco smoke, I suggest that this piece of information be followed up with a non-jargon description of reported immediate effects. RF 2601:204:D980:38C8:3582:C79D:5EA0:39D (talk) 03:34, 13 May 2019 (UTC)
- For content about POW camps I would need sources to add content to Nicotine#History,_society,_and_culture.
- At low amounts, it has a mild analgesic effect.[7] Is that what you want added? Source says "At low doses, it is a weak analgesic, but at high doses, it causes tremors and seizures."[8] QuackGuru (talk) 01:48, 14 May 2019 (UTC)
- I referred to POW camps only to explain my reasoning, I'm not actually asking for a POW section. Yes, I would not be against mentioning the analgesic effect. Generally, smokers report a relaxed feeling, increased alertness, mild euphoria, stress relief, etc. I suggest replacing the second sentence of the article with a sentence along these lines, seeing as the second sentence is a bit technical for an introduction and is already present word-for-word in the pharmacology section. RF 66.115.169.223 (talk) 11:11, 14 May 2019 (UTC)
- I added it to the body first. I also added it to the lede that follows the order of content that is in the body. QuackGuru (talk) 16:19, 14 May 2019 (UTC)
- Alright. I also added to the first paragraph to mention that it's the active ingredient in cigarettes. Before it kind of read like nicotine was some pharmaceutical product developed to help people quit smoking, when in fact it's the thing in cigarettes in the first place. Listed some common effects as well.RF 66.115.169.223 (talk) 20:02, 14 May 2019 (UTC)
- Usually a citation is needed for adding new content.
- Others will review the edits and decide if any of the edits were an improvement. QuackGuru (talk) 21:00, 14 May 2019 (UTC)
- Alright. I also added to the first paragraph to mention that it's the active ingredient in cigarettes. Before it kind of read like nicotine was some pharmaceutical product developed to help people quit smoking, when in fact it's the thing in cigarettes in the first place. Listed some common effects as well.RF 66.115.169.223 (talk) 20:02, 14 May 2019 (UTC)
- I added it to the body first. I also added it to the lede that follows the order of content that is in the body. QuackGuru (talk) 16:19, 14 May 2019 (UTC)
- I referred to POW camps only to explain my reasoning, I'm not actually asking for a POW section. Yes, I would not be against mentioning the analgesic effect. Generally, smokers report a relaxed feeling, increased alertness, mild euphoria, stress relief, etc. I suggest replacing the second sentence of the article with a sentence along these lines, seeing as the second sentence is a bit technical for an introduction and is already present word-for-word in the pharmacology section. RF 66.115.169.223 (talk) 11:11, 14 May 2019 (UTC)
- I would argue the foremost reason it has been used extensively is rather the effects it has once it's been processed pharmacologically by the body. People didn't use cigarettes as currency in POW camps because they wanted to stop their addiction, they did it because cigarettes make people feel good, (so they were actually using it to continue their addiction.) This is what makes it appealing and thus addicting and widespread. An introduction should include the most basic, essential points about a subject. This seems to me to be an essential piece of information because it's the whole reason the molecule is of interest in the first place. The lack of any mention of the reason nicotine has appeal to people contrasted with extensive reference to risks makes the introduction read a little like anti-drug propaganda. Just stating that it's a "potent parasympathomimetic alkaloid" is not very useful for most people who want to understand the reason people inhale tobacco smoke, I suggest that this piece of information be followed up with a non-jargon description of reported immediate effects. RF 2601:204:D980:38C8:3582:C79D:5EA0:39D (talk) 03:34, 13 May 2019 (UTC)
I hadn't read any of the responses in the thread until now. Your argument about nicotine w.r.t. people using cigarettes as currency in POW camps because they feel good makes no sense. Cigarettes are not nicotine. NRT does not produce euphoria. Seppi333 (Insert 2¢) 22:28, 14 May 2019 (UTC)
- Rather than the argument not making sense, you seem to have misunderstood it. Nicotine replacement therapy is not designed to provoke the effects of a dose of nicotine taken in by smoking tobacco products. Rather, it seems to me that it is designed to provide a certain low level of nicotine to an addict, in order to make the brutal cessation of smoking less difficult. Obviously, it would be unlikely for this kind of dose to produce the same effects as a cigarette. Cigarettes are not nicotine, but it's been established that nicotine is the main active ingredient in them. Therefore, the observed fact that cigarettes are seen as desirable by humans indicates a strong likelihood that nicotine produces pleasant effects, which are also commonly reported. RF2601:204:D980:38C8:C9A0:7594:DD29:4C1D (talk) 08:27, 18 May 2019 (UTC)
- No, I understood. Nicotine by itself does not produce euphoria in a significant number of people (e.g., me), as stated and cited in the article. From personal experience, high doses of NRT produce a rather unpleasant experience if anything. That said, nicotine is the compound that makes tobacco addictive, it's not the only or primary psychoactive constituent though. Seppi333 (Insert 2¢) 17:03, 18 May 2019 (UTC)
- When a smoker quits, they feel really terrible; but longitudinal studies show that once they get over the withdrawal, their mood is better than it was when they were nicotine-dependent. Similarly, if people take up smoking their average mood worsens. Some research (cited in the article) suggests that the pleasant effect of nicotine (like other central nervous system stimulants) is that it temporarily relives nicotine withdrawal; "Smokers have worse mood than they would have if they were not nicotine-dependent; they experience normal moods only immediately after smoking." (if you have suggestions for a clearer way to express this content, they would be very welcome). A lack of pleasant effects would thus be expected in anyone not physically dependent on nicotine. Some published trials using nicotine patches in non-nicotine users had really high quit rates, as the volunteers, like Seppi333, found the effects really unpleasant. Unpleasantness in initiating nicotine use is commonly reported
, though a euphoric effect that is rapidly removed by habituation would explain why nicotine use often escalates(it wouldn't explain it better than the withdrawal relief mechanism, Occam's razor). HLHJ (talk) 04:03, 20 May 2019 (UTC)
- When a smoker quits, they feel really terrible; but longitudinal studies show that once they get over the withdrawal, their mood is better than it was when they were nicotine-dependent. Similarly, if people take up smoking their average mood worsens. Some research (cited in the article) suggests that the pleasant effect of nicotine (like other central nervous system stimulants) is that it temporarily relives nicotine withdrawal; "Smokers have worse mood than they would have if they were not nicotine-dependent; they experience normal moods only immediately after smoking." (if you have suggestions for a clearer way to express this content, they would be very welcome). A lack of pleasant effects would thus be expected in anyone not physically dependent on nicotine. Some published trials using nicotine patches in non-nicotine users had really high quit rates, as the volunteers, like Seppi333, found the effects really unpleasant. Unpleasantness in initiating nicotine use is commonly reported
"youth" vs. " in their mid-twenties and younger"
QuackGuru, there was a consensus on WP:MED for not using vague terms like "youth". "in their mid-twenties and younger" or "until their late twenties" is not much longer and is much more likely to produce an impression that accurately reflects MEDRS. Most people who get addicted to nicotine do so before their mid-20s, so this is highly relevant information. I've added a really concise version. HLHJ (talk) 03:44, 20 May 2019 (UTC)
- After reading one of the sources I could not verify the claim. "such as those under 25 years old.[citation needed]" QuackGuru (talk) 20:28, 20 May 2019 (UTC)
QuackGuru, you deleted three citations and replaced them with a citation-needed tag], with the comment "too many citations". I will replace a smaller number of citations if you want. Does this meet your approval?
You also replaced "such as those under ~25" with "such as those under 25 years old"; the tilde, meaning "approximately", was used for brevity per your previous objection. The Surgeon General said "until about age 25"; he makes it clear that this is approximate, as people's brains mature at different rates. HLHJ (talk) 20:33, 20 May 2019 (UTC)
- The citation to the PDF file for the Surgeon General does not work. QuackGuru (talk) 20:40, 20 May 2019 (UTC)
- In what way? HLHJ (talk) 20:49, 20 May 2019 (UTC)
- "E-Cigarette Use Among Youth and Young Adults: A Report of the Surgeon General" (PDF). United States Department of Health and Human Services. Surgeon General of the United States. 2016. pp. 1–298.
- I clicked on the citation for the PDF file and it was a dead link. QuackGuru (talk) 20:50, 20 May 2019 (UTC)
- In what way? HLHJ (talk) 20:49, 20 May 2019 (UTC)
- I just clicked on your link above and it loaded, can't explain this disrepancy. Actually, I didn't use that link in the citations you deleted; I used this link, which is an index linking to the full report, the executive summary, the factsheet, the press release, etc.. The citation without the link would still be valid; it contains enough bibliographic information to find the source easily (see WP:dead link). A quick response to this sort of problem is using Template:Dead link or some such. HLHJ (talk) 21:06, 20 May 2019 (UTC)
- QuackGuru, I see you've replaced my three citations with the one you gave above, leaving the citation-needed tag. I'd prefer my link, as most people will probably not want to read through a 298-page report, but will read a summary. I'd be OK with having both links as "links to summaries, full report". Can you also not access the other two sources, including the Surgeon General's advisory that says "until about age 25"? Could you please explain why you think the cn tag is needed? HLHJ (talk) 21:39, 20 May 2019 (UTC)
- "such as those under 25 years old.[28][verification needed]" What page verifies the claim? I can't find where the source verifies the claim. Just one citation is needed when a page number is given. QuackGuru (talk) 22:57, 20 May 2019 (UTC)
- Page 2 of 2.5, not counting references, in the advisory. It's the only occurrence of the numeral "25". "Nicotine exposure during adolescence can harm the developing brain – which continues to develop until about age 25". The other sources use vaguer terms, but support the statement (e.g. "The use of products containing nicotine poses dangers to youth, pregnant women, and fetuses" in the full report). In an attempt to speed this up, I've re-added the advisory citation and tilde. HLHJ (talk) 23:23, 20 May 2019 (UTC)
- See "Nicotine exposure during adolescence can harm the developing brain – which continues to develop until about age 25". [9] The does not verify it is one of the vulnerable groups. Nicotine can be harmful at older age too. The other source explicitly verifies the claim for youth. QuackGuru (talk) 01:26, 21 May 2019 (UTC)
- I'd say that if something can harm your brain, that is a vulnerability. A group vulnerable to brain harm is a vulnerable group. You've removed the edits discussed in this section altogether.
- I was actually drafting a removal of the "in youth"/"in [specify somehow])" content, as I had made an edit to add content that I thought covered the material better. It said "There is debate over whether nicotine initiates cancers. It promotes tumour growth and may promote tumour progression.[31][32][33][34] Nicotine is a teratogen;[35][30][36][37][38] it harms brain growth and development, which continues into the early to mid-20s.[28][39]". This replaced "The International Agency for Research on Cancer indicates that nicotine does not cause cancer.[31] Nicotine has been shown to produce birth defects in some animal species, but not others;[32] consequently, it is considered to be a possible teratogen in humans.[32]" Counting even the square brackets, my version added five more characters, and it reflects the current literature much more accurately. I was very careful not to significantly extend anything but the citations in length. You reverted this with "too much deytail again for lede". As I said in my earlier edit, I think the old content violates WP:MEDANIMAL. It also directly contradicts recent MEDRS sources. Can you please explain what sort of content would meet with your approval, in sufficient detail that I can write content that you will not reject? HLHJ (talk) 04:26, 21 May 2019 (UTC)
- "I'd say that if something can harm your brain, that is a vulnerability." is not what the source states. If that was the case then every age group is a vulnerable group. That is not the case. "Nicotine induces behavioral stimulation in animals." is allowed as long as it is made clear the content states it in "animals". You've been arguing for months now and content that I believe fails verification is continuing to be added to the article. Any more changes can be done by a RfC or gain consensus. QuackGuru (talk) 19:20, 21 May 2019 (UTC)
- See "Nicotine exposure during adolescence can harm the developing brain – which continues to develop until about age 25". [9] The does not verify it is one of the vulnerable groups. Nicotine can be harmful at older age too. The other source explicitly verifies the claim for youth. QuackGuru (talk) 01:26, 21 May 2019 (UTC)
- Page 2 of 2.5, not counting references, in the advisory. It's the only occurrence of the numeral "25". "Nicotine exposure during adolescence can harm the developing brain – which continues to develop until about age 25". The other sources use vaguer terms, but support the statement (e.g. "The use of products containing nicotine poses dangers to youth, pregnant women, and fetuses" in the full report). In an attempt to speed this up, I've re-added the advisory citation and tilde. HLHJ (talk) 23:23, 20 May 2019 (UTC)
- "such as those under 25 years old.[28][verification needed]" What page verifies the claim? I can't find where the source verifies the claim. Just one citation is needed when a page number is given. QuackGuru (talk) 22:57, 20 May 2019 (UTC)
- QuackGuru, I see you've replaced my three citations with the one you gave above, leaving the citation-needed tag. I'd prefer my link, as most people will probably not want to read through a 298-page report, but will read a summary. I'd be OK with having both links as "links to summaries, full report". Can you also not access the other two sources, including the Surgeon General's advisory that says "until about age 25"? Could you please explain why you think the cn tag is needed? HLHJ (talk) 21:39, 20 May 2019 (UTC)
Nicotine causality and cancer
The current lede says "The International Agency for Research on Cancer indicates that nicotine does not cause cancer.[29] Nicotine has been shown to produce birth defects in some animal species, but not others;[30] consequently, it is considered to be a possible teratogen in humans.[30] ". The first statement is, I recall, based on a 2007 review; the second source is a Data Bank entry citing animal studies from the 70s and 80s, not revised since 2009. I think that the statements are out-of-date and omit important context. I replaced this with
There is debate over whether nicotine initiates cancers. It promotes tumour growth and may promote tumour progression.[1][2][3][4] Nicotine is a teratogen;[5][6][7][8][9] it harms brain growth and development, which continues into the early to mid-20s.[10][11]
...such that the total lede length was about the same. My change was reverted. What are people's reasons for preferring the one or the other? HLHJ (talk) 05:05, 4 August 2019 (UTC)
New content
@HLHJ: Can you qualify the following statement you added with an explanation or example of how it is harmful, as described by the source you cited? However, nicotine is harmful to non-users.
I don't have time to go through the ref right now and I don't particularly like to see vague statements like this in an article. Seppi333 (Insert 2¢) 09:08, 20 May 2019 (UTC)
- Sure, I'll do my best. QuackGuru feels that the lede is too long, which is why I was so overly-succint. I will try and supply the information without unduly lengthening the lede; if I fail, I'll expect to hear about it here. 19:14, 20 May 2019 (UTC)
- FWIW, the lead of this article seems fine in terms of length right now since long articles are supposed to have 4 paragraphs in the lead. Once this article has been fully expanded, this article's lead section should be about as long as amphetamine's, which is a bit longer than the nicotine's lead section as of right now. Seppi333 (Insert 2¢) 19:24, 20 May 2019 (UTC)
"However, nicotine is harmful to non-users." failed verification. QuackGuru (talk) 20:30, 20 May 2019 (UTC)
- Thank you for the info on what I'm aiming for, Seppi333. I'm working on it, trying to keep the lede length ~unaltered. QuackGuru, Schraufnagel has an entire section headed "It ignores nicotine and its harmful effects". This seems to support the statement that nicotine is harmful. The qualification is added because obviously if it helped you quit smoking, that would be a net win, and a reduction in harm, per the last-but-one sentence. HLHJ (talk) 20:39, 20 May 2019 (UTC)
- Sorry, Seppi, I thought I'd have time to finish this but I have not. Schraufnagel 2015 says that nicotine consumption acutely raises blood pressure, heartrate, and rates of erectile dysfunction in non-users (checked through to the sources). No-one seems to have done long-term follow up on such studies, or long-term studies on people who use NRTs as you do (welcoming correction, if you know of any?). Nicotine has been found to cause gastrointestinal disorders in regular users.[12] Multi-month exposure to nicotine worsens a variety of diseases[13] and reduces fertility, in animal studies.[14] There is some more complementary content which I added and QG removed (see section above). I had added more detail on some of this to the "contraindications" section. There's also some vaguer content on relative risk which I want to research more and tighten up: The ideal course of action for smokers is to quit all nicotine use, but use of nicotine alone is substantially less harmful than smoking.[15] For those quitting smoking, NRT reduces net harm.[16] For someone initiating nicotine use, comparison to smoking risks is irrelevant.[6] Feel free to add any of this content, I will get back to it when I can. HLHJ (talk) 04:42, 21 May 2019 (UTC)
References
- ^ Cite error: The named reference
carcinogenicitywas invoked but never defined (see the help page). - ^ "Does nicotine cause cancer?". European Code Against Cancer. World Health Organization – International Agency for Research on Cancer. Before October 25th 2014[1]. Retrieved 23 January 2019.
{{cite web}}: Check date values in:|date=(help); External link in|date= - ^ Grando, Sergei A. (15 May 2014). "Connections of nicotine to cancer". Nature Reviews Cancer. 14 (6): 419–429. doi:10.1038/nrc3725. PMID 24827506.
{{cite journal}}:|access-date=requires|url=(help) - ^ Cardinale, A; Nastrucci, C; Cesario, A; Russo, P (January 2012). "Nicotine: specific role in angiogenesis, proliferation and apoptosis". Critical reviews in toxicology. 42 (1): 68–89. doi:10.3109/10408444.2011.623150. PMID 22050423.
{{cite journal}}:|access-date=requires|url=(help) - ^ Kohlmeier, KA (June 2015). "Nicotine during pregnancy: changes induced in neurotransmission, which could heighten proclivity to addict and induce maladaptive control of attention". Journal of developmental origins of health and disease. 6 (3): 169–81. doi:10.1017/S2040174414000531. PMID 25385318.
{{cite journal}}:|access-date=requires|url=(help) - ^ a b Cite error: The named reference
Schraufnagel2015was invoked but never defined (see the help page). - ^ Bruin, Jennifer E.; Gerstein, Hertzel C.; Holloway, Alison C. (2010-04-02). "Long-Term Consequences of Fetal and Neonatal Nicotine Exposure: A Critical Review". Toxicological Sciences. 116 (2): 364–374. doi:10.1093/toxsci/kfq103. ISSN 1096-6080. PMC 2905398. PMID 20363831.
Briefly, nicotine has been clearly established as a neuroteratogen that compromises the development of critical neural pathways in the developing brain... Overall, the evidence provided in this review overwhelmingly indicates that nicotine should no longer be considered the safe component of cigarette smoke. In fact, many of the adverse postnatal health outcomes associated with maternal smoking during pregnancy may be attributable, at least in part, to nicotine alone.
- ^ "Electronic Cigarettes: What's the bottom line??" (PDF). US Centers for Disease Control.
- ^ England, Lucinda J.; Kim, Shin Y.; Tomar, Scott L.; Ray, Cecily S.; Gupta, Prakash C.; Eissenberg, Thomas; Cnattingius, Sven; Bernert, John T.; Tita, Alan Thevenet N.; Winn, Deborah M.; Djordjevic, Mirjana V.; Lambe, Mats; Stamilio, David; Chipato, Tsungai; Tolosa, Jorge E. (31 December 2010). "Non-cigarette tobacco use among women and adverse pregnancy outcomes". Acta Obstetricia et Gynecologica Scandinavica. 89 (4): 454–464. doi:10.3109/00016341003605719. ISSN 1600-0412. PMC 5881107. PMID 20225987.
The use of any products containing nicotine likely will have adverse effects of fetal neurological development.
- ^ Cite error: The named reference
SG_advisorywas invoked but never defined (see the help page). - ^ Cite error: The named reference
SG_2016was invoked but never defined (see the help page). - ^ Chu, KM; Cho, CH; Shin, VY (2013). "Nicotine and gastrointestinal disorders: its role in ulceration and cancer development". Current pharmaceutical design. 19 (1): 5–10. PMID 22950507. Retrieved 20 May 2019.
- ^ Lee, PN; Fariss, MW (April 2017). "A systematic review of possible serious adverse health effects of nicotine replacement therapy". Archives of toxicology. 91 (4): 1565–1594. doi:10.1007/s00204-016-1856-y. PMID 27699443. Retrieved 20 May 2019.
- ^ "Nicotine". United States National Library of Medicine – Toxicology Data Network. Hazardous Substances Data Bank. Retrieved 23 January 2019.
- ^ Nicotine without smoke: Tobacco harm reduction. London: Royal College of Physicians. 2016. p. 151. ISBN 978-1-86016-600-6.
- ^ Cite error: The named reference
mediatedwas invoked but never defined (see the help page).
Nicotine addiction
If "nicotine addiction" is typed into the WP search box, it brings the reader to this article, on the section regarding breast cancer links. 107.77.215.65 (talk) 20:21, 16 June 2019 (UTC)
Quality of Article
- The quality of this article isn't that great. Statements from sources of wildly varying quality are strewn throughout the article, and especially the summary could be way more summarizing. I'm not competent to review sources and claims, but there's contradictions in the article itself.
- Simple factual errors have gone uncorrected for long times – 2 to 7 µg/kg is not 20 to 70 millionths in weight, as anyone with an idea of how powers of ten work might have noticed. (I'm correcting that by removing the bogus verbal reproduction.)
- The article itself is partially very repetitive. — Preceding unsigned comment added by Marcusmueller ettus (talk • contribs) 12:45, 27 October 2019 (UTC)
MEDRS?
Hey QuackGuru, let's discuss the last addition/revert[10] ![]()
The entry does not look like MEDRS to me part of the entry does not look MEDRS to me, particularly the Research section, which contains exactly one reference about humans, the rest is about in vitro studies, and most are primary or "trends" papers. I would propose to consider this entry more under WP:SCIRS, and eventually divide human vs animal studies if you'd like to make stuff clearer. I'll also look for stronger sources on this effect, it's probably mentioned in one of the sources already here. If that doesn't sound good for you, what would you propose? --Signimu (talk) 01:21, 4 November 2019 (UTC)
- PS: I didn't mention the "failed verification", but I'm not sure why you considered that, given all the infos could be found in either the title or the sources top paragraphs, if this remains a major issue, I can provide quotes --Signimu (talk) 01:23, 4 November 2019 (UTC)
- Would this source be better for nicotine and POMC interaction? PMID 23632083 --Signimu (talk) 01:36, 4 November 2019 (UTC)
- Upon better reading the entry, I think I understand a bit better how it's organized. I think my additions would be a better fit for the pharmacology section, using the new ref above, but I'm not an expert in pharmaco, so it would be better if someone else reviews. What would you think of something like that?
- "Nicotine activates via β4* nAChR the POMC neurons in the arcuate nucleus and subsequently MC4 receptors on second order neurons in the paraventricular nucleus of the hypothalamus, modulating feeding inhibition."[1]
References
- ^ Picciotto, MR; Mineur, YS (January 2014). "Molecules and circuits involved in nicotine addiction: The many faces of smoking". Neuropharmacology. 76 Pt B: 545–53. doi:10.1016/j.neuropharm.2013.04.028. PMC 3772953. PMID 23632083.
--Signimu (talk) 01:52, 4 November 2019 (UTC)
- I restarted the section using one review. PMID 23632083 is a review and thus useful. It is very technical and it can be tricky to rewrite the content when it is very complicated. QuackGuru (talk) 02:26, 4 November 2019 (UTC)
- Yes I agree, so that's why I simply paraphrased what they wrote about POMC neurons above ;-) I'll leave more technical expansions to other more competent editors than me in the domain --Signimu (talk) 09:56, 4 November 2019 (UTC)
- Ah I saw your addition and new source, great! Thanks a lot for taking the time
 I'll maybe add just a precision about the pathway succinctly as above --Signimu (talk) 10:03, 4 November 2019 (UTC)
I'll maybe add just a precision about the pathway succinctly as above --Signimu (talk) 10:03, 4 November 2019 (UTC)
- Yes I agree, so that's why I simply paraphrased what they wrote about POMC neurons above ;-) I'll leave more technical expansions to other more competent editors than me in the domain
- I restarted the section using one review. PMID 23632083 is a review and thus useful. It is very technical and it can be tricky to rewrite the content when it is very complicated. QuackGuru (talk) 02:26, 4 November 2019 (UTC)
Excessive citations requested
I think the [citation needed] near the forms of recreational nicotine products (more specifically, chewing tobacco and snus; snuff is already cited, but apparently that source isn't good enough) is absurd. I realize that it may not meet the criteria for common knowledge, but the fact that the forms of tobacco listed have articles of their own should be enough. If the lack of citation really bothered whoever made this edit, they could have easily used any of the sources from the articles about the forms of tobacco in question to verify that they are indeed used recreationally. These calls for citation do not help the reader in any way, and their inclusion is indicative of the editor's devotion to rules without understanding why they exist. There is no controversy, debate, or confusion about the fact that people use chewing tobacco or that it contains nicotine. It may not be common knowledge in the way that we all know the sky is blue, but there is certainly no need for the reader to treat the claim that people use chewing tobacco recreationally as dubious. What other way would they use it? Medically? As a decoration? I'm putting this in the talk section instead of editing it myself because I know it would be reverted instantly. If a citation is truly necessary, I have already provided a simple solution for finding one. 47.7.136.252 (talk) 14:25, 3 September 2019 (UTC)
Diabetes
The citations to this paper should be monitored in the future, about nicotine effect on melanocortin system promoting diabetes mellitus. It's already having a lot of publicity in scientific vulgarization magazines, I can bet it will be included in a future review soon enough.[1] Indeed, there is already increasing evidence of a link between cigarettes smoking and increasing risk of metabolic syndrome in humans,[2] but here they identified a pathway from nicotine (rather than all the other chemical components in cigarettes). --Signimu (talk) 10:51, 4 November 2019 (UTC)
References
- ^ Duncan, A; Heyer, MP; Ishikawa, M; Caligiuri, SPB; Liu, XA; Chen, Z; Vittoria Micioni Di Bonaventura, M; Elayouby, KS; Ables, JL; Howe, WM; Bali, P; Fillinger, C; Williams, M; O'Connor, RM; Wang, Z; Lu, Q; Kamenecka, TM; Ma'ayan, A; O'Neill, HC; Ibanez-Tallon, I; Geurts, AM; Kenny, PJ (October 2019). "Habenular TCF7L2 links nicotine addiction to diabetes". Nature. 574 (7778): 372–377. doi:10.1038/s41586-019-1653-x. PMID 31619789.
{{cite journal}}: Unknown parameter|lay-url=ignored (help) - ^ Chiolero, A; Faeh, D; Paccaud, F; Cornuz, J (April 2008). "Consequences of smoking for body weight, body fat distribution, and insulin resistance". The American journal of clinical nutrition. 87 (4): 801–9. doi:10.1093/ajcn/87.4.801. PMID 18400700.
New nicotine image
What is this image doing in this article? There is a bit of red added to the image. How does one know what is the structure of a pronated nicotine made with a base of benzoic acid? QuackGuru (talk) 21:58, 5 November 2019 (UTC)
- Maybe Theislikerice can help us clarify what was the purpose of adding this image? --Signimu (talk) 09:09, 6 November 2019 (UTC)
- The purpose is to show the structure of protonated nicotine (e.g. which nitrogen is protonated) together with the structure of benzoate. Structure here means Lewis structure, not 3D structure. If you do an image search, you see there is some confusion about what nicotine salts are (e.g. this image) --Theislikerice (talk) 19:54, 7 November 2019 (UTC)
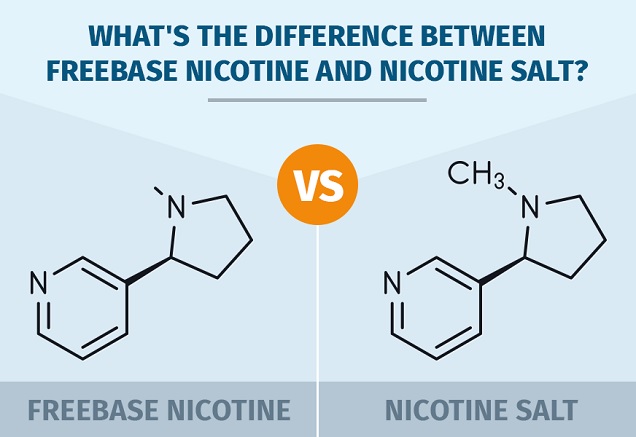{kind=link}
There is not enough content about the salts to justify an image. QuackGuru (talk) 13:15, 14 November 2019 (UTC)
- I think an image of the conjugate acid (protonated nitrogen) as compared to the neutral form is useful. I'd be fine with no counter-anion, or just generic "X–". I added a cited note about the sign change and that this is specifically related to the protonation (not the specific counter-anion), so now there is an encyclopediac detail that an image comparing the two forms would support. It also likely changes the molecular geometry, though I don't have a ref handy. And "which nitrogen is protonated" is indeed something that is not obvious (though it does match the general pattern of pKa for 3° amine vs pyridine). DMacks (talk) 04:34, 20 November 2019 (UTC)
- There is a paper on spectroscopy of nicotine salts supporting the protonation at the tertiary amine (Perfetti, T. A. (1983). Structural study of nicotine salts. Beiträge zur Tabakforschung/Contributions to Tobacco Research, 12(2), 43-54.) and a crystal structure of nicotine gentisate presented at a conference last year showing a hydrogen bond between the carboxylate group of the organic acid and the quaternary nitrogen of protonated nicotine (https://www.coresta.org/sites/default/files/abstracts/2019_ST15_YangJi.pdf). The specific counterion is not important, but it is relevant to show an organic anionic species because it can release the free base nicotine in the gas phase by reversing the acid/base reaction (nicotine chloride would not release nicotine into the gas phase upon heating but nicotine benzoate does).Theislikerice (talk) 13:24, 10 January 2020 (UTC)
- Commons has File:Nicotine molecule ball from xtal.png whose ref (1971 x-ray of salicylate) concurs. DMacks (talk) 13:42, 10 January 2020 (UTC)
- There is a paper on spectroscopy of nicotine salts supporting the protonation at the tertiary amine (Perfetti, T. A. (1983). Structural study of nicotine salts. Beiträge zur Tabakforschung/Contributions to Tobacco Research, 12(2), 43-54.) and a crystal structure of nicotine gentisate presented at a conference last year showing a hydrogen bond between the carboxylate group of the organic acid and the quaternary nitrogen of protonated nicotine (https://www.coresta.org/sites/default/files/abstracts/2019_ST15_YangJi.pdf). The specific counterion is not important, but it is relevant to show an organic anionic species because it can release the free base nicotine in the gas phase by reversing the acid/base reaction (nicotine chloride would not release nicotine into the gas phase upon heating but nicotine benzoate does).Theislikerice (talk) 13:24, 10 January 2020 (UTC)
{kind=link}
Covid-19
A small though respectable French study has suggested that nicotine may have an inhibitory effect on Covid-19 symptoms: https://www.theguardian.com/world/2020/apr/22/french-study-suggests-smokers-at-lower-risk-of-getting-coronavirus Is it worth adding this to the article, or is it too tentative? --Ef80 (talk) 15:01, 22 April 2020 (UTC)
Incorrect additions
A number of new content has been added to the article that does not meet Wikipedia’s standards for sourcing or accuracy. Random e-cigarette websites are not reliable sources of information for a science article. ecigarette-politics.com in particular is not a reliable source. It states on its website "I am not sympathetic to any restrictions on EV-related products of any type, except quality controls as existing for example in normal EU consumer product regulations; nor to EV businesses or groups who support any such restrictions. E-Cigarette regulations cost lives." I think there's a clear case for deleting any facts that rely on this source.
Additionally, some of the information is false: “Nicotine is not much addictive on its own,” in addition to needing to be rephrased to standard English, is also contradicted by the article info box, which states that the dependence liability of nicotine is “High.”
I am aware of research that shows that nicotine, administered on its own, is not nearly as addictive as it is in the form of tobacco. I think this is what Machinexa was referring to. But being less addictive in relative terms is not the same as being “not much addictive” in absolute terms, and the article’s existing, reliable sources make clear that nicotine itself is highly addictive in absolute terms.
Wallnot (talk) 15:43, 27 June 2020 (UTC)
Reverted all article changes by Machinexa, as many/all of the changes to text were supported by references that did not meet WP:MEDRS standards. Additionally, extraordinary statements (nicotine is not much addictive) require extraordinary citation support. David notMD (talk) 17:15, 27 June 2020 (UTC)
No serious dispute
Nicotine can harm adolescent brain development.[1][2][3]
References
- ^ Yuan, Menglu; Cross, Sarah J.; Loughlin, Sandra E.; Leslie, Frances M. (2015). "Nicotine and the adolescent brain". The Journal of Physiology. 593 (16): 3397–3412. doi:10.1113/JP270492. ISSN 0022-3751. PMC 4560573. PMID 26018031.
- ^ Peterson, Lisa A.; Hecht, Stephen S. (2017). "Tobacco, e-cigarettes, and child health". Current Opinion in Pediatrics. 29 (2): 225–230. doi:10.1097/MOP.0000000000000456. ISSN 1040-8703. PMC 5598780. PMID 28059903.
- ^ "Why Is Nicotine Unsafe for Kids, Teens, and Young Adults?". Centers for Disease Control and Prevention. 11 March 2019.
There is no serious dispute per WP:ASSERT and is it common knowledge the harms to brain development. Numerous WP:MEDRS compliant sources verify the exact same wording. QuackGuru (talk) 15:53, 27 May 2020 (UTC)
- QuackGuru, I assume this is addressed to User:Zvi Zig? Their edit summary points to the previous discussion at Talk:Nicotine/Archive_2#Cognitive_harms_in_lede; it would be helpful to address the objections raised there. There is some proposed text at the end of that section, and User:HLHJ added claims to the lede in May 2019. QuackGuru actually removed this language in this edit with the summary "too much deytail again for lede". Zvi Zig removed some language which eventually got restored in this edit in May 2020, so I presume the proposed text did not achieve consensus. Given the reliable sources cited on both sides, perhaps the lede simply needs to say that authorities disagree on whether or not the evidence on this matter is definitive. There has been text on this subject in the "Adverse effects" section in the past, and it could go into detail (perhaps in a new subsection) explaining the differing secondary or tertiary opinions.
- Claims of "common knowledge" have no place in resolving medical questions. Wikipedia:Common knowledge explains why. -- Beland (talk) 17:58, 29 May 2020 (UTC)
- The text that was recently removed from the body and lede was in the article for quite some time. There is literally hundreds of reviews that verify the same or similar claim. The previous lede was getting too long. Some content was eventually restored to the lede and summarised in the body. QuackGuru (talk) 01:57, 30 May 2020 (UTC)
- Stating in the lede that "authorities disagree on whether or not the evidence on this matter is definitive." is not supported by any source presented. Unsourced content should not be added to the lede. Among top-tier sources such as the CDC[11] and WHO[12] there is no disagreement. Also see the FDA: "As adolescent brains are still developing, nicotine exposure during youth and young adulthood can change the way the brain works, leading to a lifetime of addiction and, in some cases, causing long-lasting effects such as increased impulsivity and mood disorders."[13] QuackGuru (talk) 15:55, 1 June 2020 (UTC)
I propose restoring both sentences[14][15] since they are accurate and neutral. The wording says it "can" not that it "will" harm adolescent brain development. There are other high-quality sources that verify similar content. For example, see on page 59 of the 2019 WHO report: "Apart from the known harmful effects of nicotine on the developing brain,...".[16] The details or debate can be expanded in the "Adverse effects" section. QuackGuru (talk) 01:57, 30 May 2020 (UTC)
- The Royal College of Physicians clearly states, "the relevance of these findings to human brain development remains uncertain".
- Source: 2016 Royal College of Physicians' report "Nicoitne Without Smoke" (P. 59). Download link: https://www.rcplondon.ac.uk/file/3563/download
- Public Health England, the leading UK public health authority, cites the Royal College of Physicians and concurs.
- Source: Evidence review of e-cigarettes and heated tobacco products 2018 A report commissioned by Public Health England (p. 60). Download link: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/684963/Evidence_review_of_e-cigarettes_and_heated_tobacco_products_2018.pdf
- Should Wikipedia present a single-sided version of the debate and ignore these respectable authorities?
- Zvi Zig (talk • contribs 04:09, 4 June 2020 (UTC)
FTR, QuackGuru has been banned from medicine articles, and will not be responding. -- Beland (talk) 22:36, 4 June 2020 (UTC)
- BTW I think it is fair to write "authorities disagree on whether or not the evidence on this matter is definitive.". I think that Wikipedia ought to allow such nuance, rather than black and white statements.
- Zvi Zig (talk • contribs 06:01, 5 June 2020 (UTC)
- I'm confused as to QG's position. Zvi Zig, I apologize for not getting back to you. Beland, thank you for the ping. I think the reasons for the difference are mainly that that the UK sources a) rely on fewer and older sources than the Surgeon-General's reviews, and b) generally refer to harms of use of NRT in smokers (harms to the smokers or their fetuses); this is clearly not a nicotine/no-nicotine comparison. Separately, could we please avoid using "adolescents", especially to include all those in their mid-20s or younger? I think it is likely to give readers the wrong impression. I suggest that our lede should include the content of this CDC public health information summary of the effects of nicotine (image, though the fourth point seems redundant). I would also welcome more recent MEDRS; 2016 is a bit old now. HLHJ (talk) 02:01, 9 July 2020 (UTC)
- The Royal College of Physician's position is not outdated, and it is clearly in line with primary sources.
- Two 2016 reports, SGR and RCP, disagreed on whether evidence of nicotine and cognitive development is conclusive. The SGR also implies the limitations of its own position:
- "Limited direct human experimental data exist on the effects of nicotine exposure from e‑cigarettes on the developing adolescent brain, but experimental laboratory data have been found to be relevant in animal models to contextualize effects in humans."
- I'm confused as to QG's position. Zvi Zig, I apologize for not getting back to you. Beland, thank you for the ping. I think the reasons for the difference are mainly that that the UK sources a) rely on fewer and older sources than the Surgeon-General's reviews, and b) generally refer to harms of use of NRT in smokers (harms to the smokers or their fetuses); this is clearly not a nicotine/no-nicotine comparison. Separately, could we please avoid using "adolescents", especially to include all those in their mid-20s or younger? I think it is likely to give readers the wrong impression. I suggest that our lede should include the content of this CDC public health information summary of the effects of nicotine (image, though the fourth point seems redundant). I would also welcome more recent MEDRS; 2016 is a bit old now. HLHJ (talk) 02:01, 9 July 2020 (UTC)
- Furthermore, the 2018 Public Health England report concurs with the 2016 RCP position.
- As discussed in the RCP report, smoking in adolescence has been associated with cognitive and attentional deficits and suggested to impact mental health, although confounding factors (such as self-selection) have not been taken into account thus far.
- In addition, if we are considering primary sources, there is evidence that nicotine does ++not++ substantially harm human cognitive development.
- "Educational achievement did not differ within twin pairs discordant for smoking, in adults and adolescents."
- Treur et al. Smoking during adolescence as a risk factor for attention problems. (2015) Biol. psychiatry
- “The (inverse) IQ–smoking association disappeared after adjustments for shared environment and genetics.”
- Wennerstad et al. Associations between IQ and cigarette smoking among Swedish male twins. Social science & medicine
- “Past smoking was not associated with significantly poorer performance than never smokers in any cognitive domain.”
- Corley et al. Smoking, childhood IQ and cognitive function in old age. (2012) Journal of Psychosomatic Research (Table 2)
- Zvi Zig (talk • contribs 03:47, 9 July 2020 (UTC)
- ^ "Electronic Cigarettes – What are the health effects of using e-cigarettes?" (PDF). Centers for Disease Control and Prevention. 22 February 2018.
Addictive - lead wording
A recent edit by Zvi Zig (no user page) changed the wording in the lead from "Nicotine is highly addictive" to "Nicotine can be highly addictive". I strongly disagree with this edit, here's why. "Addictive", as defined by the OED, means "(of a substance or activity) causing or likely to cause someone to become addicted." This implies that the substance has the intrinsic capacity to cause addiction, unlike other substances and activities which do not possess this intrinsic property at all or to a lesser extent and thus not typically causing addiction. Intercourse can be addictive but the vast majority of individuals engaging in the activity do not struggle with being addicted to it, unlike nicotine where a much higher proportion of users consuming it become addicted to it. The neurobiology of the reward pathway (I suspect through the habenula) enables nicotine to create an addiction and thus the phrasing should be "is addictive" rather than "can be addictive" with the latter being reserved for substances and activities which do not commonly or easily form addiction. Please do correct me if there is a precedent for this wording, I could find little pertinent discussion in the talk archive. Revanchist317 (talk) 09:43, 4 June 2020 (UTC)
- Nicotine is highly dependent on the delivery system. Even intravenous nicotine is not that readily self-administered addictive review. Nicotine, as a chemical, is not necessarily "highly likely" to cause addiction in all. NRT is classified by the FDA to have a low risk of abuse or addiction and is sold OTC. A 2018 PHE report concludes, "The addictiveness of nicotine depends on the delivery system." Nicotine is very different from chemicals which are blanketly highly addictive.
- Zvi Zig (talk • contribs 05:55, 5 June 2020 (UTC)
- Alright, that's fine by me then. In the light of this evidence, I completely agree with the current wording of the lead. Cheers
- Revanchist317 (talk) 06:39, 5 June 2020 (UTC)
- Revanchist317, Zvi Zig, could we replace "Nicotine can be highly addictive, depending on how it is used" with something like "Nicotine is highly addictive, unless used in slow-release forms"? This is no longer and gives more information. The thing is, nothing is addictive if delivered slowly enough. Rapid reward is an intrinsic part of addiction. See also CDC summary in image above. HLHJ (talk) 02:05, 9 July 2020 (UTC)
- Agree.Zvi Zig (talk • contribs 03:43, 9 July 2020 (UTC)
- Agree. Revanchist317 (talk) 20:23, 9 July 2020 (UTC)
- Modified per consensus. Thank you both. HLHJ (talk) 02:07, 11 July 2020 (UTC)
- Agree. Revanchist317 (talk) 20:23, 9 July 2020 (UTC)
- Agree.Zvi Zig (talk • contribs 03:43, 9 July 2020 (UTC)
- Revanchist317, Zvi Zig, could we replace "Nicotine can be highly addictive, depending on how it is used" with something like "Nicotine is highly addictive, unless used in slow-release forms"? This is no longer and gives more information. The thing is, nothing is addictive if delivered slowly enough. Rapid reward is an intrinsic part of addiction. See also CDC summary in image above. HLHJ (talk) 02:05, 9 July 2020 (UTC)
Insulin resistance
This page states “insulin resistance” as a side effect of nicotine but when I followed the link to the source (https://en.wikipedia.org/wiki/File:Side_effects_of_nicotine.png#Summary) I could not find insulin resistance listed in the side effects.
{kind=link}
To my knowledge, the effect of nicotine on insulin resistance is unclear. Some studies show that it increases insulin resistance, other studies (for example: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3520975/) show that it decreases insulin resistance.
Should this be changed or mentioned on this page? — Preceding unsigned comment added by MoMoBig (talk • contribs) 13:22, 25 July 2020 (UTC)
WP:POV
this article requires a wholesale overhaul; reads like a t r u t h ad rather than a legitimate drug article on Wikipedia. Yes, nicotine is addictive! ...and other countless psychotropics with propensity for dependence receive objective unbiased evaluations on their respective pages without morally charged qualifiers, ya know, suitable for an online encyclopedia. 2605:6000:EB40:3A00:7D5A:90D9:B0A6:E635 (talk) 05:36, 13 September 2020 (UTC)KillaCamInDaFlesh
- To me it reads like a well sourced, well written encyclopedic article on a well researched topic. I see no pov violations. - DVdm (talk) 08:35, 13 September 2020 (UTC)
Lede statement that nicotine causes distress
A statement in the lede says: "Nicotine dependence causes distress.[1]"
On the other hand, as per an NEJM review, "Nicotine induces pleasure and reduces stress and anxiety."[2]
Most recent Mendelian randomization indicates no effect in either direction.[3]
The page should reflect WP:NPOV.
Zvi Zig (talk • contribs 05:05, 14 September 2020 (UTC)
References
- ^ Parrott AC (March 2006). "Nicotine psychobiology: how chronic-dose prospective studies can illuminate some of the theoretical issues from acute-dose research" (PDF). Psychopharmacology. 184 (3–4): 567–76. doi:10.1007/s00213-005-0294-y. PMID 16463194. S2CID 11356233.
- ^ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2928221/.
{{cite web}}: Missing or empty|title=(help) - ^ https://bmjopen.bmj.com/content/4/10/e006141.
{{cite web}}: Missing or empty|title=(help)
- Yes, nicotine induces pleasure and reduces stress and anxiety, and nicotine dependence causes distress. I think that the immediate stress and anxiety reduction effects could be mentioned in the Nicotine#Recreational subsection. DVdm (talk) 09:00, 14 September 2020 (UTC)
- The best evidence available, from Mendelian randomization, supports a net neutral effect.
[1]Zvi Zig (talk • contribs 04:50, 15 September 2020 (UTC)... future studies should therefore employ methods that enable stronger causal inference, such as Mendelian randomization (MR)... Two studies that have used MR have found no evidence to support a causal association between smoking and depression and anxiety, while another found evidence to suggest that smoking was associated with lower odds of depression during pregnancy. The results of these studies suggest that observational findings of an association of smoking status with later psychological distress may be a result of shared vulnerability, residual confounding, or reverse causality (eg, psychological distress associated with later smoking behavior).
- The best evidence available, from Mendelian randomization, supports a net neutral effect.
N-nitrosonornicotine
We should probably reach a consensus about the mention of N-nitrosonornicotine, or NNN, in the lead. Whilst I orignially agreed with User:DVdm, upon a second look I have to admit I misread the study. The study in question, Knezevich et al, 2013, link below, investigated the formation of NNN from deuterium-marked precursors incubated in human saliva. While they did note that NNN formed from nornicotine, their conclusion was that "only traces of [pyridine-D4]NNN were found in samples incubated with [pyridine-D4]nicotine and sodium nitrite." [sic]. This appears to suggest that the presence of nornicotine itself is dangerous and leads to the formation of NNN, rather than nicotine itself. Therefore, I have to side with User:Zvi Zig, although I disagree with the justification for removal on the grounds that these were ex vivo findings. Whilst that's true, measuring this in vivo would be borderline impossibe and using human saliva is as good as one gets with this research, so I don't think it breaks WP:MEDANIMAL. I would argue this should be removed from the lead section, although maybe it should be added to the article Health effects of tobacco or elsewhere as this study seems relevant for tobacco smoking, rather than for nicotine itself. What do you think? Revan (talk) 16:55, 30 October 2020 (UTC)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3611998/
- I agree. The importance the ex-vivo factor is that nicotine is metabolized in the body, and therefore trace findings could be further reduced.Zvi Zig (talk • contribs 05:54, 8 November 2020 (UTC)
Nicotine a parasympathomimetic?
Nicotine is introduced as a parasympathomimetic. However, it has both sympathetic and parasympathetic effects, which cancel each other out (besides for in the cardiovascular system where the sympathetic prevails). https://opentextbc.ca/anatomyandphysiology/chapter/15-4-drugs-that-affect-the-autonomic-system/ .
Other reviews state "nicotine is a sympathomimetic". https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2946180 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3195407
Any input on this? Zvi Zig (talk • contribs 06:37, 19 October 2020 (UTC)
- I have not received a response - if anyone can show that I missed something please comment - but nicotine is a clearly much broader agonist than a parasympathomimetic. It is certainly not a "potent" parasympathomimetic, as sympathomimetic effects ultimately prevail. Zvi Zig (talk • contribs 07:39, 10 November 2020 (UTC)
In header "Nicotine itself is associated with some health harms"
which isn't what the associate link says, it says foetal harm and "...the effect of nicotine on the developing adolescent brain, which will develop differently under the influence of nicotine than without it." The summary is too broad, any objection to me modifying this to mention foetal development and adolescent's brains? 79.75.105.69 (talk) 12:26, 29 November 2020 (UTC)
- I agree.
- Furthermore, outside of fetal development, there is no consensus on harm. For example, Royal College of Physicians states, “use of nicotine alone, in the doses used by smokers, represents little if any hazard to the user”.[2] And with regards to rodent studies of nicotine affecting to adolescent cognitive development, it concludes, "The relevance of these findings to human brain development remains uncertain." Zvi Zig (talk • contribs 18:37, 29 November 2020 (UTC)
- Thanks, so what do you think of the original "Nicotine itself is associated with some health harms.[29]" becoming "Nicotine by itself is may cause fetal harm, and possibly alter brain development in adolescents.[29]" - acceptable? 79.75.102.149 (talk) 19:08, 29 November 2020 (UTC)
- That looks like an accurate reflection of the sources.Zvi Zig (talk • contribs 19:18, 29 November 2020 (UTC)
- However, considering WP:MEDANIMAL guidelines
In vitro studies and animal models serve a central role in research, and are invaluable in determining mechanistic pathways and generating hypotheses. However, in vitro and animal-model findings do not translate consistently into clinical effects in human beings. Where in vitro and animal-model data are cited on Wikipedia, it should be clear to the reader that the data are pre-clinical, and the article text should avoid stating or implying that reported findings hold true in humans.
- it should probably say that this is based on animal research.Zvi Zig (talk • contribs 23:45, 29 November 2020 (UTC)
- In the original link https://en.wikipedia.org/wiki/Nicotine#cite_note-Edgar2013-29 there's no mention of animals I can see, your link https://www.rcplondon.ac.uk/file/3563/download?token=Mu0K_ZR0 fails to download so I can't read it. Can you point me to why animals are relevant? 79.75.123.136 (talk) 10:11, 30 November 2020 (UTC)
- Interesting. The link downloads a PDF when I tried it. Alternatively, this link reads within the browser.
- Here is the relevant paragraph on page 59
Research from animal studies suggests that fetal exposure to nicotine may lead to adverse postnatal health consequences63 and that cognitive function and development are adversely affected by nicotine exposure during both the fetal and the adolescent periods.64 The relevance of these findings to human brain development remains uncertain, however. There is evidence that smoking in adolescence is associated with cognitive and attentional impairments in later life, and possibly an increased risk of mental health problems,65 but it is difficult to exclude the effects of confounders of this association in the observational studies available.
- Zvi Zig (talk • contribs 05:27, 1 December 2020 (UTC)
- @Zvi Zig, I'm sorry I've been so busy I've not been able to get back to this - if you wish would you care to pick suitable phrasing and amend the article? TBH you seem to have a better grasp on all this than I. If you can't, I'll try to get back to it sometime.79.76.128.13 (talk) 11:12, 6 December 2020 (UTC)
- Okay. Fetal harm is already addressed in that paragraph. For the animal evidence of nicotine adversely affecting cognitive development in adolescence, in humans, past smoking is not associated with reduced cognitive ability, in studies adjusting for childhood IQ.[3] Therefore, while I don't think the animal studies should get weight where human studies exist, because they have been mentioned by the RCP report, I think they should be mentioned.Zvi Zig (talk • contribs 22:18, 6 December 2020 (UTC)
- @Zvi Zig, I'm sorry I've been so busy I've not been able to get back to this - if you wish would you care to pick suitable phrasing and amend the article? TBH you seem to have a better grasp on all this than I. If you can't, I'll try to get back to it sometime.79.76.128.13 (talk) 11:12, 6 December 2020 (UTC)
- In the original link https://en.wikipedia.org/wiki/Nicotine#cite_note-Edgar2013-29 there's no mention of animals I can see, your link https://www.rcplondon.ac.uk/file/3563/download?token=Mu0K_ZR0 fails to download so I can't read it. Can you point me to why animals are relevant? 79.75.123.136 (talk) 10:11, 30 November 2020 (UTC)
- Thanks, so what do you think of the original "Nicotine itself is associated with some health harms.[29]" becoming "Nicotine by itself is may cause fetal harm, and possibly alter brain development in adolescents.[29]" - acceptable? 79.75.102.149 (talk) 19:08, 29 November 2020 (UTC)
References
- ^ Fluharty, Meg; Taylor, Amy E.; Grabski, Meryem; Munafò, Marcus R. (January 2017). "The Association of Cigarette Smoking With Depression and Anxiety: A Systematic Review". Nicotine & Tobacco Research. 19 (1): 3–13. doi:10.1093/ntr/ntw140.
- ^ p. 125 https://www.rcplondon.ac.uk/file/3563/download?token=Mu0K_ZR0
- ^ https://www.cambridge.org/core/services/aop-cambridge-core/content/view/3D14E86FFD2156D5E3ABA7C4A91F21EA/S0033291717001489a.pdf/healthy_cognitive_ageing_in_the_lothian_birth_cohort_studies_marginal_gains_not_magic_bullet.pdf
Harm to bystanders
The statement in the lead, "Nicotine is potentially harmful to non-users" is highly contentious.
It is contentious whether nicotine harms users,[1][2][3] certainly nonusers.
Public Health England's calculates that: "EC release negligible levels of nicotine into ambient air with no identified health risks to bystanders."[4]
Therefore, this statement appears to be a violation of Wikipedia's neutrality policy, WP:NPOV. Zvi Zig (talk • contribs 07:13, 11 December 2020 (UTC)
References
- ^ Royal College of Physicians. "Nicotine Without Smoke -- Tobacco Harm Reduction". p. 125. Retrieved 30 September 2020.
Use of nicotine alone, in the doses used by smokers, represents little if any hazard to the user.
- ^ Douglas, Clifford E.; Henson, Rosie; Drope, Jeffrey; Wender, Richard C. (July 2018). "The American Cancer Society public health statement on eliminating combustible tobacco use in the United States: Eliminating Combustible Tobacco Use". CA: A Cancer Journal for Clinicians. 68 (4): 240–245. doi:10.3322/caac.21455. PMID 29889305. S2CID 47016482. Retrieved 30 September 2020.
It is the smoke from combustible tobacco products—not nicotine—that injures and kills millions of smokers.
- ^ Dinakar, Chitra; O’Connor, George T. (6 October 2016). "The Health Effects of Electronic Cigarettes". New England Journal of Medicine. 375 (14): 1372–1381. doi:10.1056/NEJMra1502466. PMID 27705269.
Beyond its addictive properties, short-term or long-term exposure to nicotine in adults has not been established as dangerous
- ^ https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/733022/Ecigarettes_an_evidence_update_A_report_commissioned_by_Public_Health_England_FINAL.pdf
Adverse Effects -- table
Missing from the table of side effects by route of administration is the fairly recently available Nicorette® "Quick Mist" throat spray. In my experience, this has some significant side effects different from those listed for other routes of administration, due to its rapid action and the possibility of heavy dosing. As this preparation has been readily available for some years (at least in my locale), I believe it should be added to the table. I will expand on this later from my desktop. 2605:8D80:480:10D0:9096:B3A2:D80F:1C0F (talk) 22:21, 14 June 2022 (UTC)
Notable S/E include (in my experience) ataxia and confusion. I should emphasize that my comment is based on OR with a statistical sample of one(!) Of course, any additions to the table will require suitable references; I hope by now there is some good research out there on this specific product.
I will add this to my "to do" list, but as usual feel free to jump in and preempt me. --D Anthony Patriarche (talk) 22:51, 14 June 2022 (UTC)
Science
What is nitine ? 181.41.70.217 (talk) 00:49, 15 September 2022 (UTC)