Wikipedia talk:Identifying reliable sources (medicine)/Archive 27
| This is an archive of past discussions on Wikipedia:Identifying reliable sources (medicine). Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |
| Archive 20 | ← | Archive 25 | Archive 26 | Archive 27 | Archive 28 | Archive 29 | Archive 30 |
No peer review
An older section on: "Wikipedians should not perform in-depth review" was removed, but now again reinstated by Jytdog. The reason it was removed was that it is unclear what it meant. In-depth as opposed to what? Is superficial review okay? And what does it mean that we should not peer review a paper? This would entail sending entries back to the publisher, something we don't do regularly. Or if the idea is that we should not actually take into account methodology or conclusions, and that makes it impossible to actually summarize the paper at all. The passage is incoherent, and I think it should be left out. Carl Fredrik 💌 📧 15:34, 27 October 2016 (UTC)
- Removal of key guidance re "don't peer review yourself"
- We have had content in this guideline for a long time, along the following lines " "Assessing evidence quality" means editors should determine quality of the type of study. Editors should not perform detailed academic peer review. Respect the levels of evidence: Do not reject a high-quality type of study (e.g., a meta-analysis) in favor of a source from lower levels of evidence (e.g., any primary source) because of personal objections to the inclusion criteria, references, funding sources, or conclusions in the higher-level source." in this guidance for a long time, and I have referred to it many times. The key sentence " was removed by CFCF in this diff.
- I went to cite this to someone yesterday and noticed it was gone. I restored it here. That was reverted by CFCF. Argh. Jytdog (talk) 15:40, 27 October 2016 (UTC)
- You make it look like this was just unceremoniously removed, but this version was stable for 4+ months, and there was initial discussion when it was removed. We have not removed the passage that says that we cannot refute high quality sources with low quality sources, but only the unclear passage about peer review. This passage implies that we can not judge bias whatsoever, which is an entirely ludicrous notion. If we follow the wording to its logical conclusion we are left with situations where we need to give junk "systematic reviews" from the journal of herbalism w/e higher status than a very well written review in science. Yes, we had an example of that up on this page roughly at the same time as this was removed! Carl Fredrik 💌 📧 15:53, 27 October 2016 (UTC)
- the notion was first introduced in 2008 in this dif by User:WhatamIdoing, and was further refined by her in this diff. This is an essential part of this guideline. With this out, you get anonymous editors critiquing the conclusions of MEDRS sources and we cannot have that - it erodes the foundation of this entire project, that we follow reliable sources. This has made me unhappy sometimes, but I have bowed to this principle, that we look at the kind of source and don't presume to critique it ourselves. Jytdog (talk) 16:07, 27 October 2016 (UTC)
- However, with it in we cannot discount even the most absurd source if it claims to be a high quality study type. If we can't review the contents to tell that it just isn't a systematic review — then we end up endorsing it.Carl Fredrik 💌 📧 16:14, 27 October 2016 (UTC)
- The last place I find this discussed here was here, back in December. Where is the discussion you are referencing? What you write above is about assessing the type of source; the removed and restored content was about assessing the contents and conclusions of the source. Do you not see the difference? Jytdog (talk) 16:17, 27 October 2016 (UTC)
- I can't find the relevant fake "systematic review" right now, but it was discussed this year, possibly somewhere else. If I recall correctly WhatamIdoing thanked me for removing the passage after a shorter debate. I find it problematic that this was unceremoniously reintroduced, especially so without discussion. Carl Fredrik 💌 📧 16:23, 27 October 2016 (UTC)
- None of that useful or speaks to the issue. Please provide a diff showing you had consensus to remove this, and please speak to the problem it addresses. Removing this opens an irresolvable can of worms. Jytdog (talk) 16:27, 27 October 2016 (UTC)
- The fact that it was stable for 4+ months implies some consensus. If we demand an RfC for every revision we aren't going to ever evolve MEDRS and will be stuck debating what "peer-review" actually is. Including this is rather what opens the can of worms. Is peer review the same as critique? Asking us not to critique articles is just crazy, and I can attest to the fact that I've never seen a content dispute where this isn't the solution. Either we forbid something nonsensical (peer-review as that applied by journals), or we forbid actually questioning if a systematic review is systematic, or we forbid something that is essential to writing the encyclopedia. It's just a nonsense passage and I don't understand where it can even be invoked. Carl Fredrik 💌 📧 16:39, 27 October 2016 (UTC)
- You have been making a lot of edits. I only noticed that this was gone yesterday. So you have no diff of consensus to remove this (of course an RfC is not required if there is discussion and a reasonable number of folks agree). And being Bold once is not a bad thing either.
- More importantly, you still seem to missing the point. It is essential to assess the type of source (is this a review or not?) and it is important to assess the quality of the journal or textbook. What is not OK, is digging into the way the review was done or whether its conclusions are valid, etc. Critiquing it like a peer-reviewer did when it was under going that process. That is absolutely not OK for editors to do. Would you please speak to that? Thanks Jytdog (talk) 17:07, 27 October 2016 (UTC)
- (edit conflict) It just doesn't make any sense to forbid detailed peer-review and allow superficial peer review. As I said, every content dispute goes into weighing sources against eachother — sometimes it's straightforward: case report vs. meta-analysis, but often it isn't. To be fair we may need to dive deep into sources, and the fact that some people do this on faulty grounds isn't a reason to disallow everyone.
- I'm trying to think of a simple example, but think of a systematic review or meta-analysis that uses a discredited or even non-existant protocol. That source is far worse than one that uses good methodology.
- By trying to save some time by telling off crazy editors that they shouldn't analyze methodology also means that sane editors can't do it when they need to. Could you give an example of where this can actually be employed?Carl Fredrik 💌 📧 17:19, 27 October 2016 (UTC)
- I do not think you are going to find consensus for that perspective. Let's see what others say. Jytdog (talk) 17:23, 27 October 2016 (UTC)
- I just see this as essentially what comes up in each any every content dispute, and is often the only recourse we have against including shitty chiropractic journal articles. Knowing what peer-review entails: this passage only discourages those that don't know what it is. Sure, that may end up being good — but it isn't correct to include a rule that is inevitably broken by everyone who knows what they're doing and invoked only for those that don't. I guess the ambiguous wording of "in-depth" helps you do that as well, but only as long as you get to judge what in-depth means. As soon as that is disputed we end up with a far worse bag of worms. Carl Fredrik 💌 📧 17:31, 27 October 2016 (UTC)
- um i have invoked this guidance many times. Many alt-med pushers try to invalidate good sources by critiquing the conclusions or how the authors got there. It goes against pretty much the whole spirit of what it means to be an anonymous editor; we don't put ourselves above the right type of sources; we follow them. Jytdog (talk) 17:35, 27 October 2016 (UTC)
- I understand that it is a nice policy to rely on when crazy people attack sources — I just don't see how it is any different to when you say that this chiropractic article that has some really shoddy methodology (say only including studies performed at OSHER centers or w/e). The passage is problematic because if we actually end up with someone who knows what it entails they can invalidate a lot of what we do to keep the encyclopedia good. Carl Fredrik 💌 📧 17:47, 27 October 2016 (UTC)
- um i have invoked this guidance many times. Many alt-med pushers try to invalidate good sources by critiquing the conclusions or how the authors got there. It goes against pretty much the whole spirit of what it means to be an anonymous editor; we don't put ourselves above the right type of sources; we follow them. Jytdog (talk) 17:35, 27 October 2016 (UTC)
- I just see this as essentially what comes up in each any every content dispute, and is often the only recourse we have against including shitty chiropractic journal articles. Knowing what peer-review entails: this passage only discourages those that don't know what it is. Sure, that may end up being good — but it isn't correct to include a rule that is inevitably broken by everyone who knows what they're doing and invoked only for those that don't. I guess the ambiguous wording of "in-depth" helps you do that as well, but only as long as you get to judge what in-depth means. As soon as that is disputed we end up with a far worse bag of worms. Carl Fredrik 💌 📧 17:31, 27 October 2016 (UTC)
- I do not think you are going to find consensus for that perspective. Let's see what others say. Jytdog (talk) 17:23, 27 October 2016 (UTC)
- The fact that it was stable for 4+ months implies some consensus. If we demand an RfC for every revision we aren't going to ever evolve MEDRS and will be stuck debating what "peer-review" actually is. Including this is rather what opens the can of worms. Is peer review the same as critique? Asking us not to critique articles is just crazy, and I can attest to the fact that I've never seen a content dispute where this isn't the solution. Either we forbid something nonsensical (peer-review as that applied by journals), or we forbid actually questioning if a systematic review is systematic, or we forbid something that is essential to writing the encyclopedia. It's just a nonsense passage and I don't understand where it can even be invoked. Carl Fredrik 💌 📧 16:39, 27 October 2016 (UTC)
- None of that useful or speaks to the issue. Please provide a diff showing you had consensus to remove this, and please speak to the problem it addresses. Removing this opens an irresolvable can of worms. Jytdog (talk) 16:27, 27 October 2016 (UTC)
- I can't find the relevant fake "systematic review" right now, but it was discussed this year, possibly somewhere else. If I recall correctly WhatamIdoing thanked me for removing the passage after a shorter debate. I find it problematic that this was unceremoniously reintroduced, especially so without discussion. Carl Fredrik 💌 📧 16:23, 27 October 2016 (UTC)
- The last place I find this discussed here was here, back in December. Where is the discussion you are referencing? What you write above is about assessing the type of source; the removed and restored content was about assessing the contents and conclusions of the source. Do you not see the difference? Jytdog (talk) 16:17, 27 October 2016 (UTC)
- However, with it in we cannot discount even the most absurd source if it claims to be a high quality study type. If we can't review the contents to tell that it just isn't a systematic review — then we end up endorsing it.Carl Fredrik 💌 📧 16:14, 27 October 2016 (UTC)
would love to see an example where you did that and got away with it. Jytdog (talk) 18:03, 27 October 2016 (UTC)
- Every single time we deny content out of chiropractic or ayurveda journals that is exactly what we do. Carl Fredrik 💌 📧 19:00, 27 October 2016 (UTC)
- That is a pretty good point. How do we identify crappy secondary sources without critiquing their methodology? If a crappy review is somehow published in a semi-reputable journal then we're SOL without deeper critique. Sizeofint (talk) 19:17, 27 October 2016 (UTC)
- No. In those cases the journal is being addressed and that is fine. Critiquing the study itself is not fine. Jytdog (talk) 19:30, 27 October 2016 (UTC)
- (edit conflict) Or even the crap put out by the Indian Ministry of AYUSH (Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homoeopathy) [1] which tells us that cold milk with sugar candy should be used for Dengue: http://ayush.gov.in/sites/default/files/CCRAS_0.pdf
- If we aren't allowed to counter this simply on the basis that it's stupid pseudoscience — we end up having to include it because it's issued by a government body. We need to allow analysis of sources methodology and claims, and to suggest we don't strikes me as incredibly naïve. Carl Fredrik 💌 📧 19:31, 27 October 2016 (UTC)
- again you are critiquing the source, not its contents. You are really not dealing with the purpose of the language you deleted. Jytdog (talk) 19:41, 27 October 2016 (UTC)
- No, I'm critiquing the content itself, the source is only bad because of its content. Carl Fredrik 💌 📧 19:47, 27 October 2016 (UTC)
- again you are critiquing the source, not its contents. You are really not dealing with the purpose of the language you deleted. Jytdog (talk) 19:41, 27 October 2016 (UTC)
- Every single time we deny content out of chiropractic or ayurveda journals that is exactly what we do. Carl Fredrik 💌 📧 19:00, 27 October 2016 (UTC)
- I am not quickly able to understand what significance this discussion has. Both versions of this content seem equivalent to me but using different words. Could someone briefly show the options? I want to know what to consider. Blue Rasberry (talk) 16:36, 27 October 2016 (UTC)
- This is the diff in question [2]. Carl Fredrik 💌 📧 16:41, 27 October 2016 (UTC)
- (edit conflict)The content that was removed by CFCF in this diff was: " Editors should not perform detailed academic peer review.".
- I restored content along those lines here: ""Assessing evidence quality" means editors should determine quality of the type of source and quality of the publication. Editors should not perform detailed academic peer review." Jytdog (talk) 16:45, 27 October 2016 (UTC)
- The sentence "Editors should not perform detailed academic peer review" has been part of our guidance for years and should be restored. It is indisputable that the job of performing any peer review should only be done by those qualified to do so. I do not accept that Wikipedia editors are qualified to do that job, otherwise we end up allowing any POV-pusher to argue that Ernst's papers are unacceptable because the pusher doesn't like his choice of sources; or that a WHO statement on abortion can't be used because the WHO isn't neutral on the subject. Believe me, I've had those arguments and the piece of guidance that stops them in their tracks is the sentence saying that they are not allowed to do their own peer review of an article. I'll be restoring that text very soon unless there are good reasons produced here not to do so. --RexxS (talk) 23:17, 27 October 2016 (UTC)
- RexxS — As it stands it is ambiguous, and what in-depth peer review means is debatable. Maybe there is some way to rephrase it to be more apt and less likely to be misunderstood? Those that actually engage in peer review understand that pretty much any critique can be interpreted as peer review, and that what is considered in-depth varies between reviewers. Carl Fredrik 💌 📧 08:05, 28 October 2016 (UTC)
- We have to be clear that editors must respect sources, and not judge content for themselves. I edit mainly plant articles, some of which are constantly subject to the addition of "herbal medicine" information, and being able to point to guidance which is clearly neutral as to content is very important. Wikipedia doesn't censor; we need to be firm that we include information in reliable sources, regardless of the opinions of any editor. Otherwise we just feed the beliefs of those who think that the "establishment" conspires to suppress inconvenient information (e.g. that free plant remedies are as good as expensive drugs produced by "big pharma"). Perhaps
Editors should not perform detailed academic peer review
could be worded differently, but it should not be removed altogether. Peter coxhead (talk) 09:19, 28 October 2016 (UTC)- I'm sorry, Carl Fredrik, it's not ambiguous, it's merely not well-defined. It will always be easier to dismiss any wiki-lawyering about the exact meaning of "in-depth peer review" than to have to argue with every POV-pusher rejecting good sources because they feel free to do their own critique of them. If someone wants to phrase it differently, then I'm amenable, but we should not be removing one of the most useful pieces of advice that we have to counter the quacks and snake-oil salesmen. --RexxS (talk) 15:26, 28 October 2016 (UTC)
- I too was surprised to see the no peer-review sentence removed for this long. I think quite a few of us missed that it had bee removed at some point. I've lost track of home many times I've cited this guideline for editors trying engage in their own personal peer-review of individual studies. I really can't see any reason why someone would want it removed as it adds additional clarity as the idea is an important part of the guideline. Either way, now that editors are becoming aware that this piece had been removed, it's pretty clear this isn't consensus to remove that line, which is really what's needed at this point if the text is going to be removed. Kingofaces43 (talk) 20:04, 28 October 2016 (UTC)
- I'm sorry, Carl Fredrik, it's not ambiguous, it's merely not well-defined. It will always be easier to dismiss any wiki-lawyering about the exact meaning of "in-depth peer review" than to have to argue with every POV-pusher rejecting good sources because they feel free to do their own critique of them. If someone wants to phrase it differently, then I'm amenable, but we should not be removing one of the most useful pieces of advice that we have to counter the quacks and snake-oil salesmen. --RexxS (talk) 15:26, 28 October 2016 (UTC)
- We have to be clear that editors must respect sources, and not judge content for themselves. I edit mainly plant articles, some of which are constantly subject to the addition of "herbal medicine" information, and being able to point to guidance which is clearly neutral as to content is very important. Wikipedia doesn't censor; we need to be firm that we include information in reliable sources, regardless of the opinions of any editor. Otherwise we just feed the beliefs of those who think that the "establishment" conspires to suppress inconvenient information (e.g. that free plant remedies are as good as expensive drugs produced by "big pharma"). Perhaps
- RexxS — As it stands it is ambiguous, and what in-depth peer review means is debatable. Maybe there is some way to rephrase it to be more apt and less likely to be misunderstood? Those that actually engage in peer review understand that pretty much any critique can be interpreted as peer review, and that what is considered in-depth varies between reviewers. Carl Fredrik 💌 📧 08:05, 28 October 2016 (UTC)
- The sentence "Editors should not perform detailed academic peer review" has been part of our guidance for years and should be restored. It is indisputable that the job of performing any peer review should only be done by those qualified to do so. I do not accept that Wikipedia editors are qualified to do that job, otherwise we end up allowing any POV-pusher to argue that Ernst's papers are unacceptable because the pusher doesn't like his choice of sources; or that a WHO statement on abortion can't be used because the WHO isn't neutral on the subject. Believe me, I've had those arguments and the piece of guidance that stops them in their tracks is the sentence saying that they are not allowed to do their own peer review of an article. I'll be restoring that text very soon unless there are good reasons produced here not to do so. --RexxS (talk) 23:17, 27 October 2016 (UTC)
Sources for accepted diagnosis
A new passage on what constitutes an accepted diagnosis was removed by Jytdog on the basis that it was a MEDMOS issue not a MEDRS issue. I strongly contest this. Portraying a diagnosis as legitimate is down to whether it is accepted by major disease ontologies or diagnostic manuals such as DSM or ICD. How to treat the diagnosis strikes me as a very clear case where one must ask which sources are reliable. As I understand it there are no qualms about the message, rather where to put it — so unless the message is in some way inaccurate it belongs here. Carl Fredrik 💌 📧 15:39, 27 October 2016 (UTC)
- Please allow disussion about this to proceed. I am copying it below. Jytdog (talk) 15:40, 27 October 2016 (UTC)
- Morgellons should not be under "hoaxes or fake". It's not real, but it's more like the prior category. It was never a hoax. Bondegezou (talk) 15:41, 27 October 2016 (UTC)
- Or we could rename the last section to "hoaxes, fakes, and false", because it is neither dubious or alternative. That is unless you equate alternative with quackery, which I guess may be legitimate. Carl Fredrik 💌 📧 15:56, 27 October 2016 (UTC)
- Morgellons should not be under "hoaxes or fake". It's not real, but it's more like the prior category. It was never a hoax. Bondegezou (talk) 15:41, 27 October 2016 (UTC)
- The content under discussion is below.
Accepted diagnoses
Disease mongering and medicalization are serious problems in medicine, and the presence of alternative or pseudoscientific diagnoses is similarly an issue. Wikipedia takes no political stance and covers both proposed diseases and alternative diagnoses, but it is important not to give undue legitimacy.
Questionable diagnoses reach from those that are:
- Proposed or plausible yet not accepted: e.g. Misophonia
- Dubious: e.g. Trichophobia, Chronic Lyme disease
- Alternative: e.g. Adrenal fatigue, Vertebral subluxation
- Hoaxes or fake: e.g. Morgellon's
- Points 3. & 4. are somewhat similar, making distinction difficult
If a diagnosis is not accepted by major medical authorities such as DSM-V, ICD-10, etc. it should not be treated as accepted and should be handled appropriately (often in the first sentence of the article). Obvious pseudoscience should be called out. Legitimate diagnoses that are misused (e.g. testosterone deficiency) should be handled similarly, but instead of being called out as false, articles should explain overuse or other issues with the diagnosis.
I had removed this in this dif and moved it to WP:MEDMOS in this dif. As I noted in my edit note, this is more a language choice thing; the content above does not discuss how to source content about health. Jytdog (talk) 15:45, 27 October 2016 (UTC)
- I disagree, because this is language choice that depends entirely on the quality of the source.Carl Fredrik 💌 📧 15:50, 27 October 2016 (UTC)
- Thanks for talking. The only sources discussed in this, are DSM and ICD, and that appears to a binary thing - a diagnosis is in them, or not. Is that the relevance to MEDRS? If so, what is going on with the 4 part set of "questionable" kinds of diagnoses? There is no discussion of sources about that. (by the way, have a look at Postpartum psychosis which I worked over last night...) Jytdog (talk) 16:10, 27 October 2016 (UTC)
- I should say the same, you did revert 4 times before engaging yourself… Right, well guidelines don't necessarily need to be sourced — and this distinction between proposed, dubious, alternative or hoax diagnoses is unique to this page. However, the idea that accepted diagnoses are listed in various diagnostic manuals isn't controversial. I think that should be on this page rather than on MEDMOS. If you dislike the selection of diagnosis types belongs I am willing to forego it, but I do think we need to better explain the way DSM and ICD etc. are employed. The list can of course be amended to include more diagnostic manuals as well, but if we've got to start somewhere. Carl Fredrik 💌 📧 16:20, 27 October 2016 (UTC)
- I wasn't asking about the sources for the 4 subcategory breakdown. I said that there is no discussion about sourcing. This is a sourcing guideline. The only sources discussed in the proposed content are DSM (specfically DSM-5) and ICD (specifically ICD-10) I moved it to MEDMOS because it seems to more of a style thing - "here iwhs how we talk about categories of diagnoses". Not - "here is how we source diagnoses". The latter would make sense here. Jytdog (talk) 16:24, 27 October 2016 (UTC)
- Okay, then I misunderstood.
- Yes DSM/ICD inclusion is binary. This means that we have a very simple situation where in order to say: "xx is a disease of y"; it needs to be in an accepted manual.
- For the other types it is slightly more difficult to choose which one a diagnosis belongs to, which is why I didn't try to clarify beyond giving examples. The reason I included that was because it seems odd to have an explanation of what sources are accepted, and then not include what to do when something is not accepted.
- It feels odd to steer away from answering the second question to MEDMOS. Maybe that is more appropriate, but it feels clunky and risks making it harder to navigate what one actually ought to do.
In any case the part about which sources are needed in order to call something a legitimate diagnosis belongs here. - Carl Fredrik 💌 📧 16:33, 27 October 2016 (UTC)
- If -- if-- folks agree that we rely on DSM/ICD for content about diagnosis, it would make sense to have content about that. DSM-5 has been controversial. Don't know about ICD-10. Let's see what others say. Jytdog (talk) 16:47, 27 October 2016 (UTC)
- I'm not saying DSM isn't controversial. However, it together with various iterations of ICD dictate which diagnoses are considered legitimate in that they are: billable; legally treatable; can give sick leave — in large parts of the world. ICD-9 and DSM-IV are still used, and ICD-11 is on its way, and those could arguably be included (the reason I didn't is because I personally never use them). ICD-8 and DSM-III and older are not really used, and include some very questionable diagnoses by modern standards (such as homosexuality), making them directly inappropriate. There is of course debate surrounding diagnostic manuals, but I don't think this addition is actually very controversial. Carl Fredrik 💌 📧 16:54, 27 October 2016 (UTC)
- As I said above, let's see what others say. I am not opposed to having content about sourcing diagnoses; but the content you generated is not that content - it is mostly about categories of uncertain diagnoses that exist outside of ones in DSM/ICD and it seems we are both unsure where that should be. Jytdog (talk) 17:11, 27 October 2016 (UTC)
- I'm not saying DSM isn't controversial. However, it together with various iterations of ICD dictate which diagnoses are considered legitimate in that they are: billable; legally treatable; can give sick leave — in large parts of the world. ICD-9 and DSM-IV are still used, and ICD-11 is on its way, and those could arguably be included (the reason I didn't is because I personally never use them). ICD-8 and DSM-III and older are not really used, and include some very questionable diagnoses by modern standards (such as homosexuality), making them directly inappropriate. There is of course debate surrounding diagnostic manuals, but I don't think this addition is actually very controversial. Carl Fredrik 💌 📧 16:54, 27 October 2016 (UTC)
- Okay, then I misunderstood.
- I wasn't asking about the sources for the 4 subcategory breakdown. I said that there is no discussion about sourcing. This is a sourcing guideline. The only sources discussed in the proposed content are DSM (specfically DSM-5) and ICD (specifically ICD-10) I moved it to MEDMOS because it seems to more of a style thing - "here iwhs how we talk about categories of diagnoses". Not - "here is how we source diagnoses". The latter would make sense here. Jytdog (talk) 16:24, 27 October 2016 (UTC)
- I should say the same, you did revert 4 times before engaging yourself… Right, well guidelines don't necessarily need to be sourced — and this distinction between proposed, dubious, alternative or hoax diagnoses is unique to this page. However, the idea that accepted diagnoses are listed in various diagnostic manuals isn't controversial. I think that should be on this page rather than on MEDMOS. If you dislike the selection of diagnosis types belongs I am willing to forego it, but I do think we need to better explain the way DSM and ICD etc. are employed. The list can of course be amended to include more diagnostic manuals as well, but if we've got to start somewhere. Carl Fredrik 💌 📧 16:20, 27 October 2016 (UTC)
- Thanks for talking. The only sources discussed in this, are DSM and ICD, and that appears to a binary thing - a diagnosis is in them, or not. Is that the relevance to MEDRS? If so, what is going on with the 4 part set of "questionable" kinds of diagnoses? There is no discussion of sources about that. (by the way, have a look at Postpartum psychosis which I worked over last night...) Jytdog (talk) 16:10, 27 October 2016 (UTC)
- Is this proposed addition more about stating whether diagnostic criteria/procedures exist to identify a particular disease in a clinical setting; or, is it more about stating whether or not the validity/existence of a particular "disease" has been established on the basis of the existence of accepted diagnostic criteria?
- If the former is the case, I have no problem with the current wording provided that a statement is added which explicitly asserts that "the existence of diagnostic criteria for a particular disease is not necessary and sufficient for that disease to be accepted as a real/accepted medical condition." Using this exact wording isn't necessary IMO; adding any assertion which is analogous to this statement is fine with me.
- I'm opposed to any addition like this if the latter is the intent behind this proposed addition to MOS:MED or MEDRS.
- The only example that I know of where there's extensive preclinical and clinical pathophysiological evidence that supports the validity of a particular disorder as a real disease, but for which diagnostic criteria do not exist, is sexual addiction. I'm sure other examples exist though. Seppi333 (Insert 2¢) 18:17, 27 October 2016 (UTC)
- Seppi333 — I don't really understand your distinction, could you clarify what you mean? Whether or not a disease is real is not the same as it being accepted. This has nothing to do with the notability of a disease, but whether the disease is generally accepted. I would define sex addiction as a proposed disease along with Video game addiction and Internet addiction. Whether or not we agree with the politics behind accepting gambling addiction and not the others is sort of beside the point, Wikipedia doesn't take that into account. Carl Fredrik 💌 📧 19:14, 27 October 2016 (UTC)
- "Sexual addiction" describes compulsive sexual behavior as an addiction. Compulsive sexual behavior is observable in humans and has been widely reported in medical literature. So, rhetorically, what I'm stating is the difference between asking "is compulsive sexual behavior a disease?" vs asking "How can compulsive sexual behavior be diagnosed clinically?"; in this context, I'm stating that the lack of diagnostic criteria for identifying compulsive sexual behavior does not imply that compulsive sexual behavior is not the manifestation of a disease. An unrelated point here about the classification of compulsive sexual behavior, assuming one acknowledges that it is the manifestation of a disease instead of a normal behavior, is the question "is compulsive sexual behavior an addiction, a form of OCD, or something else?"
- Extensive reports of compulsive sexual behavior in humans in medical literature is part what I was referring to when I said there's "clinical evidence" supporting the validity of sexual addiction as a real disease. The other clinical evidence that I was referring to is based upon neuropsychological (i.e., operant reinforcement and incentive salience), neuroimaging (i.e., activation of specific components of the reward system), and rather limited molecular neurobiological evidence in humans, which is fully consistent with the far more comprehensive evidence derived from animal research, on the pathophysiology of compulsive sexual behavior, which happens to be almost identical to the pathophysiology of a drug addiction. Seppi333 (Insert 2¢) 20:12, 27 October 2016 (UTC)
- For starters ICD doesn't include clear diagnosic criteria, so it can impossibly explain how to diagnose a disease. It isn't up to Wikipedia to decide whether a disease is actually real or not — nor does it make a disease fake just because it isn't widely accepted. However, the fact that it isn't accepted is pretty important when it comes to how we should treat the article. Sexual addiction may very well be accepted as a diagnosis in the future, but it is not now (see WP:CRYSTALBALL). Any article on such proposed disorders should explain this, preferably in the first few sentences. The article on sexual addiction does this well, explaining it in its second paragraph. This addition to MEDRS is mainly intended to make sure this happens, as it is sometimes resisted. A recent debate at talk:misophonia concerned whether we refer to misophonia as a disease or a proposed disease. Since it's not covered in any diagnostic manual/ontology it ultimately landed at proposed (which understandably impacted the style a lot), but not before requiring much deliberation and being at least on report to a notice-board. This guideline change could save much time by simply having something to point to, instead of having to go through tedious (and ultimately pointless and time-consuming) deliberations. Carl Fredrik 💌 📧 20:26, 27 October 2016 (UTC)
- My point wasn't that Wikipedia editors should determine whether or not a disease is real based upon their own knowledge of and personal opinions on the subject. My point was that Wikipedia editors should not use the DSM-5 and ICD-10 as the sole basis to determine whether or not a disease is real; a disease necessarily must be identified as such prior to the establishment of diagnostic criteria for that disease. Seppi333 (Insert 2¢) 22:15, 28 October 2016 (UTC)
- For starters ICD doesn't include clear diagnosic criteria, so it can impossibly explain how to diagnose a disease. It isn't up to Wikipedia to decide whether a disease is actually real or not — nor does it make a disease fake just because it isn't widely accepted. However, the fact that it isn't accepted is pretty important when it comes to how we should treat the article. Sexual addiction may very well be accepted as a diagnosis in the future, but it is not now (see WP:CRYSTALBALL). Any article on such proposed disorders should explain this, preferably in the first few sentences. The article on sexual addiction does this well, explaining it in its second paragraph. This addition to MEDRS is mainly intended to make sure this happens, as it is sometimes resisted. A recent debate at talk:misophonia concerned whether we refer to misophonia as a disease or a proposed disease. Since it's not covered in any diagnostic manual/ontology it ultimately landed at proposed (which understandably impacted the style a lot), but not before requiring much deliberation and being at least on report to a notice-board. This guideline change could save much time by simply having something to point to, instead of having to go through tedious (and ultimately pointless and time-consuming) deliberations. Carl Fredrik 💌 📧 20:26, 27 October 2016 (UTC)
- Seppi333 — I don't really understand your distinction, could you clarify what you mean? Whether or not a disease is real is not the same as it being accepted. This has nothing to do with the notability of a disease, but whether the disease is generally accepted. I would define sex addiction as a proposed disease along with Video game addiction and Internet addiction. Whether or not we agree with the politics behind accepting gambling addiction and not the others is sort of beside the point, Wikipedia doesn't take that into account. Carl Fredrik 💌 📧 19:14, 27 October 2016 (UTC)
- I would not want Wikipedia to act as if DSM and ICD were the only possible disease ontologies. They're clearly not. They have their controversies. They make choices. We do need to be cautious about fictitious or "alternative" conditions and treat those appropriately, but that doesn't mean treating ICT and DSM as omniscient. Bondegezou (talk) 20:38, 27 October 2016 (UTC)
- I agree that they're not omniscient, which is why I've flagged for adding more of them, and originally included the "etc". However they are extremely important, and I think we ought to mention them, and the fact that any diagnosis listed in them is akin to being "official".
- I personally think DSM-V was a bad move compared to DSM-IV in that it medicalizes everyday life, but I don't think Wikipedia should take this stance — because it is profoundly political and not in line with WP:NPOV.
- Bondegezou — do you have any other suggestions for ontologies to include? Preferably ones that are used in clinical practice and supported by at least some government? Carl Fredrik 💌 📧 20:43, 27 October 2016 (UTC)
- There are other ontologies, like the much used SNOMED-CT or the older GALEN, but they're more designed to be computer readable, so they're doing a different sort of job and are not as usable or accessible as ICD for our purposes.
- This paper is an example of a critique of DSM and ICD. Bondegezou (talk) 20:51, 27 October 2016 (UTC)
- You can also, of course, look at Diagnosis code, Medical classification and Template:Medical classification! Bondegezou (talk) 20:53, 27 October 2016 (UTC)
- I am aware of those ontologies, however the paper is new to me (thanks). My point was more related to whether you considered any to be relevant for mention here? I know several governments are behind SNOMED-CT, but it is difficult to import to Wikipedia because it maintains database rights (it was bought by NLM from a private organization and requires licencing to use). Carl Fredrik 💌 📧 20:58, 27 October 2016 (UTC)
- It is difficult to import SNOMED, but some Wikipedians will have access to it, so we can still mention it. Bondegezou (talk) 21:46, 27 October 2016 (UTC)
- The problem is not so much of access as that by retaining database rights for commercial use in their licence we cannot import it systematically. We can add SNOMED-CT IDs to articles on a one-by-one basis, but we can never add them all (even if we did it one-by-one) because that would be a violation of the licence. However, as it is widely used we ought to be able to add it to the list. Carl Fredrik 💌 📧 21:55, 27 October 2016 (UTC)
- It is difficult to import SNOMED, but some Wikipedians will have access to it, so we can still mention it. Bondegezou (talk) 21:46, 27 October 2016 (UTC)
- I am aware of those ontologies, however the paper is new to me (thanks). My point was more related to whether you considered any to be relevant for mention here? I know several governments are behind SNOMED-CT, but it is difficult to import to Wikipedia because it maintains database rights (it was bought by NLM from a private organization and requires licencing to use). Carl Fredrik 💌 📧 20:58, 27 October 2016 (UTC)
- You can also, of course, look at Diagnosis code, Medical classification and Template:Medical classification! Bondegezou (talk) 20:53, 27 October 2016 (UTC)
essays
I don't believe essays should link in the body of a policy or guideline which is confusing for some editors who seem to think essays carry weight beyond the input and especially opinion of a single or a few editors. (Littleolive oil (talk) 22:33, 30 October 2016 (UTC))
- What exactly do you mean? Example? Alexbrn (talk) 22:42, 30 October 2016 (UTC)
- See my changes here:
- I believe the language of MEDRS is too critical to create and allow links within the body of the guideline to an essay where some editors probably newer ones will believe the essay carries equal weight to the guideline itself which of course it cannot. It doesn't matter if the essay seems to be in agreement with the guideline. That essay has not been vetted by the community or it would have guideline or policy status. If we open the door in the guideline itself to links to essays we agree with, we will have a hard time explaining the removal of essays we don't agree with. Links to essays belong in the see also section or have, traditionally, in my experience.(Littleolive oil (talk) 23:03, 30 October 2016 (UTC))
- The WP:PAGs generally are bristling with links to essays (see WP:NPOV e.g.). So if you're proposing this as a general principle it would seem to run counter to settled consensus. Essays are prominently labelled as not being policy so a reader should be fine with knowing their status. There are some very useful essays we should link to e.g. WP:WHYMEDRS. Alexbrn (talk) 23:10, 30 October 2016 (UTC)
- I agree we should link to essays; I just don't think it should be in the body of a policy or guideline. Since there is an implied consensus to do so I'll leave it at that. I hadn't noticed and I think its a very bad idea, but that's just my position.(Littleolive oil (talk) 23:52, 30 October 2016 (UTC))
- I had a similar problem recently over a section of the MOS that used the {{main}} template to link to a Help: page. That implied that the MOS section was a WP:Slly ary of the Help: page - i.e. the Help page dictated the content of the MOS section. In the end the only way to settle the consequent differences of opinion was to run an RfC to "promote" the Help: page to guideline status. Given my experience with that, I'm not at all sure that linking to essays from the MOS enjoys consensus, although it does seem a common enough practice. The problem with essays, of course, is that they are a mixed bag, some very good advice, others very dubious (and no way of marking the difference!). The problem with implied consensus, of course, is that it only holds until someone challenges it.
- My advice would be to discuss a given link to an essay on its merits, when challenged, rather than assuming a blanket consensus in favour or against for every case. In this instance, Wikipedia:Identifying and using primary sources is a pretty useful essay, IMHO, and I wouldn't worry about it being linked from the MOS. Obviously, other editors may have different, equally valid, views. --RexxS (talk) 01:48, 31 October 2016 (UTC)
- I agree we should link to essays; I just don't think it should be in the body of a policy or guideline. Since there is an implied consensus to do so I'll leave it at that. I hadn't noticed and I think its a very bad idea, but that's just my position.(Littleolive oil (talk) 23:52, 30 October 2016 (UTC))
- The WP:PAGs generally are bristling with links to essays (see WP:NPOV e.g.). So if you're proposing this as a general principle it would seem to run counter to settled consensus. Essays are prominently labelled as not being policy so a reader should be fine with knowing their status. There are some very useful essays we should link to e.g. WP:WHYMEDRS. Alexbrn (talk) 23:10, 30 October 2016 (UTC)
- I believe the language of MEDRS is too critical to create and allow links within the body of the guideline to an essay where some editors probably newer ones will believe the essay carries equal weight to the guideline itself which of course it cannot. It doesn't matter if the essay seems to be in agreement with the guideline. That essay has not been vetted by the community or it would have guideline or policy status. If we open the door in the guideline itself to links to essays we agree with, we will have a hard time explaining the removal of essays we don't agree with. Links to essays belong in the see also section or have, traditionally, in my experience.(Littleolive oil (talk) 23:03, 30 October 2016 (UTC))
- The two diffs presented in the OP are the same diff. There were two separate edits.
- Neither edit was helpful. Jytdog (talk) 22:05, 31 October 2016 (UTC)
- The essay was added to the article/guideline under the "see also" section. Right? I don't understand your cmt., Jytdog. I had used the wrong link and have replaced it. Thanks for the heads up on that.
- Rexx. Thank you. You are identifying the situation as I see it, although I'm not sure the most fundamental problem is with how useful the essay is but, that it is an essay at all. Given the range of usefulness of essays, I'm not convinced the best way to deal with essays is to add them to individual sections which leaves the essay, however useful it is or isn't, in place, unless someone notices it. I also wonder if its less trouble to designate a specific place in a policy or guideline for essays rather than have to have an RfC later and all that entails, if there is a dispute. However either solution is possible seems to me. Thanks for your perspective. My internet connection is going in and out so I may not be able to respond.(Littleolive oil (talk) 00:03, 1 November 2016 (UTC))
- WP:CIR. Look at your own diffs for pete's sake; i described exactly what you actually did above. Jytdog (talk) 01:27, 1 November 2016 (UTC)
I'm afraid you are confusing competence with differences of opinion on the way to do something. Further you are linking to an essay. WP: CIR as means to support your behaviour and as we have been discussing essays are opinions and do not carry the weight of policies and guidelines. You said that your cmt made no sense; sure it does for anyone who reads the comment which follows in which I explain the mistake. I mistakenly added the same link twice then fixed that mistake, the same kind of mistake made my numerous editors in my experience even at the arbitration level. No one gets in a flap over this kind of thing so you might want to chill a little. You are now edit warring the link. What the heck is that about? I contested the placement of an essay, I added that essay to the "see also" section of the guideline which sat along with multiple other "see also" information. The essay is not the guideline; it is at best an addendum. Even so, I have no problem with it being added; I was suggesting it belonged in another place. End of story. I have also agreed there is more than one way to deal with this situation. I think you need to let this go and drop the stick.(Littleolive oil (talk) 02:02, 1 November 2016 (UTC))
- Again, look at your actual diffs, as I provided and described them above. In the first one, you added a shortcut to a section of this guideline (WP:MEDDEF) to See also; that is not a link to an essay. Then you deleted 2 shortcuts and deleted the link to an essay. For pete's sake. Jytdog (talk) 02:19, 1 November 2016 (UTC)
I see what you are referring to. I'm going to assume from there that you and I do not understand each other and leave it at that. This is going nowhere. Best. (Littleolive oil (talk) 02:24, 1 November 2016 (UTC))
- You are completely misrepresenting what you actually did. Again. You never moved the essay to See also but that is what you said you did here. Jytdog (talk) 02:28, 1 November 2016 (UTC)
Actually I see what you are saying and I missed that. I moved the wrong link to "see also" and then removed both links in the section. The confusion was that when I clicked on the top of the page I was linking to the essay and did not realize I was missing the shortcut. D'oh. My discussion was on the use and placement of the essay so I stand by that but I apologize for misunderstanding what you were getting at.(Littleolive oil (talk) 02:37, 1 November 2016 (UTC))
- Thank you for finally paying attention to what you actually did. What a waste of time. Jytdog (talk) 02:44, 1 November 2016 (UTC)
- Jytdog try exercising graciousness. We all waste each other's time. No one here is perfect. (Littleolive oil (talk) 02:47, 1 November 2016 (UTC))
- LOO try exercising some carefulness. There are now diffs throughout of WP of you saying X and doing Y. Of course no one is perfect but no one should have to tell you four times that your edits and your words don't match. Especially not on a guideline, which as you noted, are very important. EspeciaJytdog (talk) 02:49, 1 November 2016 (UTC)s
- Care is something we all need to deal with. This wasn't a case of edits and words not matching, so let's characterize this correctly. This was a case of me not understanding what you were getting at, of the language you were using not making sense to me. When people talk they can misunderstand each other. I have seen you apologize multiple times on Wikipedia, and you have had editors accept your apologies as honest. Please extend the same to others. And ....I have been mischaracterized in multiple situations and I remember and have documented for myself where those places are. (Littleolive oil (talk) 03:08, 1 November 2016 (UTC))
- LOO try exercising some carefulness. There are now diffs throughout of WP of you saying X and doing Y. Of course no one is perfect but no one should have to tell you four times that your edits and your words don't match. Especially not on a guideline, which as you noted, are very important. EspeciaJytdog (talk) 02:49, 1 November 2016 (UTC)s
- Jytdog try exercising graciousness. We all waste each other's time. No one here is perfect. (Littleolive oil (talk) 02:47, 1 November 2016 (UTC))
Policy
I recently had an admin inform me the MEDRS is a policy but has an outdated "guideline tag" on it. Is this accurate? Primergrey (talk) 01:43, 15 December 2016 (UTC)
- No, like the rest of the Manual of Style, it's a guideline, but one that is strongly enforced in the absence of circumstances that would make it impractical. --RexxS (talk) 14:13, 15 December 2016 (UTC)
- Thanks Primergrey (talk) 14:48, 15 December 2016 (UTC)
Future of magic links
In case anyone is interested, a decision has apparently been made to remove all magic links, which includes PMID and ISBN.
I can't find any discussions where consensus was established. There is Requests for comment/Future of magic links on Mediawiki; a mailing list post by Legoktm in October; a thread on phabricator, T148274; and a request to approve a bot to remove them. Spinningspark left a note about the bot request on WP:VPP. SarahSV (talk) 16:13, 22 December 2016 (UTC)
- see Wikipedia_talk:WikiProject_Medicine/Archive_89#PMID_magic_links Jytdog (talk) 16:19, 22 December 2016 (UTC)
- Jytdog, thank you. The assumption is that the PMID magic link isn't used much. I don't know about anyone else, but I use it a lot because I don't use citation templates. SarahSV (talk) 16:23, 22 December 2016 (UTC)
- User:SlimVirgin i use it on talk pages. it was on one of the gratuitously, wonderfully, easy things here. Jytdog (talk) 16:42, 22 December 2016 (UTC)
- Jytdog, I agree. Also agree with the other points you made in the November discussion. SarahSV (talk) 16:59, 22 December 2016 (UTC)
- User:SlimVirgin i use it on talk pages. it was on one of the gratuitously, wonderfully, easy things here. Jytdog (talk) 16:42, 22 December 2016 (UTC)
- Jytdog, thank you. The assumption is that the PMID magic link isn't used much. I don't know about anyone else, but I use it a lot because I don't use citation templates. SarahSV (talk) 16:23, 22 December 2016 (UTC)
Very well and clearly written guidelines
I must thank all the contributors of these guidelines and to the very concept of creating these guidelines. I am reading these guidelines now and I must mention that they are very useful and making very clear and understandable points. One feels a kind of joy while reading so exhaustive and well written guidelines. Once again many thanks to all the contributors. Thank you. -- Abhijeet Safai (talk) 10:32, 24 February 2017 (UTC)
Graphics in #Books
For reference, here is the graphic (and associated caption) under discussion:

I am a little concerned that the graphic in Wikipedia:Identifying_reliable_sources_(medicine)#Books seem to be misleading. It appears to conflate the "level" of a book with its quality or reliability. To be sure, it is unlikely that a low level textbook (e.g., the popular press book) is reliable under MEDRS, but it seems like a mistake to say that professional level books are higher quality than graduate level or college level books for example. The text of the guideline emphasizes the need for a book to be up to date, more than the specific level at which it is aimed. Professional books can be out of date, and current graduate level textbooks can be sources of the highest quality. So, for now I am removing the graphic. This material seems to be better conveyed by the written text, which the graphic fails to summarize. Sławomir Biały (talk) 10:51, 2 April 2017 (UTC)
- In general the image holds true, and varying quality between different types of books is unrelated to whether they are up-to-date or not. This image doesn't touch upon whether it is better to use a graduate level textbook from 2005 over a undergraduate textbook from 2015. Do you have any suggestions for improvements in wording or in the image to clarify this? As far as I'm concerned the problem is in no way alleviated by removing a clear and informative image. Carl Fredrik talk 12:58, 2 April 2017 (UTC)
- Really there are two issues with the image. One of which is the timeliness of the material, discussed in the text. The other is that it is quite simply a mistake to equate the intended level of a book with its factual reliability. I am sure that there are professional level books on chiropractic, for example, that would not be regarded as reliable medical sources. Sławomir Biały (talk) 13:00, 2 April 2017 (UTC)
- Well, your second statement that you call a "mistake" generally holds true: that there is a correlation between intended level of a book and factual reliability/accuracy. Of course it does not always hold, but taken together with the section on academic publishers vs. predatory or popular publishers: you end up with a workable definition. I agree it might be inaccurate to equate this with quality, but it is a usable measure for suitability in most medical articles.
- When it comes to pseudoscience, such books are seldom published by recognized publishers. Carl Fredrik talk 13:05, 2 April 2017 (UTC)
- I'd like to add what I think is probably the most important point: the images are there to guide interest and maintain an ease of understanding. The text is more important — and to me if one more reader looks at the images and gets the jist of what we mean, rather than not reading this "dry" and "boring" guideline, then I'm happy. Better to have a superficial understanding of something than to have no understanding at all — that is what the images are for. The text will always trump the images.
- Please come with suggestions and I can incorporate them quickly, the files are svgs and easily editable. Carl Fredrik talk 13:10, 2 April 2017 (UTC)
- I am not convinced that college level and graduate level textbooks are generally less reliable than professional level books. Sławomir Biały (talk) 13:16, 2 April 2017 (UTC)
- Really there are two issues with the image. One of which is the timeliness of the material, discussed in the text. The other is that it is quite simply a mistake to equate the intended level of a book with its factual reliability. I am sure that there are professional level books on chiropractic, for example, that would not be regarded as reliable medical sources. Sławomir Biały (talk) 13:00, 2 April 2017 (UTC)
- I am inclined to agree with Sławomir Biały here. The broad generalization that texts pitched at an undergraduate or graduate versus a "professional" audience are inherently or presumptively of lower quality is not really justified. At best, it might be a tolerable rule of thumb in an all-else-being-equal situation—but I've never yet encountered a situation where all else is really equal. On balance, the graphic is more likely to mislead than to assist. As with all sources, we should be examining textbooks and monographs on a case-by-case basis to determine if their use is appropriate (or sufficient) to support a given claim in a particular article. TenOfAllTrades(talk) 14:46, 2 April 2017 (UTC)
- There is an incredible overestimation of the way general editors rely on guidelines here. Most (if not all) editors go by gut instinct, only consulting guidelines when there is an issue. Once again I will clarify that in general the heuristic holds, and only rarely is it not applicable. Thus it is a useful image to convey the most basic understanding of the guideline — that there exist different levels of published works, some of which are more suitable than others.
- The other major issue here is that: removing the image does not solve any issues — the confusion is still present in the text. If you are suggesting we clarify that this is only a rule of thumb — fine, I agree that may be apt, but removing all visual aids indiscriminately is not helpful.
- Please suggest some improvements instead, this image has been in the guideline for 8+ months without any critique. If we really need to remove it, it isn't something that will happen on a whim with a 1 paragraph justification on the talk-page. Carl Fredrik talk 16:14, 2 April 2017 (UTC)
- I don't see how the length of time that the image was in the guideline is relevant. Was there some RfC that preceded its introduction? Otherwise one editor may justifiably remove such an image just as another may add it, without either editor being accused of behaving whimsically. Certainly, if I had been notified eight months ago, I would have voiced my concern at the time.
- I am not aware of any specific number of paragraphs that must accompany the removal of a recently-added policy item, but I note an inability to find any paragraphs that specifically accompanied its addition. On the contrary, the only paragraph I can find in the archive that specifically addresses the new images argues against their inclusion:
- It often seems a good idea to replace editorial judgement based on descriptive guidelines by a flowchart or other deterministic set of rules, but it very rarely turns out to be a good idea in practice. It leads to wikilawyering about the precise boundaries of the choices in the "rules". It discourages editors, especially new editors, from trying to understand the guidance provided, instead encouraging them to follow their interpretation of the "rules". — @Peter coxhead:
- I note that these reasons are complementary to my own positive reasons, and also independently support the removal of the graphic. Let me note yet another reason the graphic is misleading: very often it is the case that textbooks at the graduate and undergraduate level are kept more up-to-date than books targeting a professional audience, because the former have a more frequent publication cycle because of the economics of the publishing industry, while the latter are much less likely to go into second and third editions and typically have a much longer cycle between editions. Sławomir Biały (talk) 17:16, 2 April 2017 (UTC)
- 3 quick points before I go to bed (will write a longer reply tomorrow):
- Stop it with the strawman about No. of paragraphs. The point is this is stable and you contest it — that isn't enough to just get rid of it.
- I disagree very strongly with the idea that images must be perfect to be included. The fact is no one knows all our policies. Not even the most experienced editor has up-to-date knowledge of all relevant policies. Images can guide both new and experienced users to better application of policies — even if they are not perfect. As long as there is an explanation that the image is not to be followed as set it stone, there really is no issue. Just point to the last sentence and then to the text, no Wikilawyering possible.
- Professional textbooks are actually quite often both published more often and are more up-to-date in medicine. This is different from other fields, but it is down to high demand on professional texts. Undergraduate or graduate textbooks often include simplifications or errors that are discredited in other sources: e.g. Precapillary sphincter — still taught in undergraduate courses today. @LT910001: Carl Fredrik talk 20:44, 2 April 2017 (UTC)
- Claims of stable version are mostly spurious. Any version is "stable" until someone notices something wrong with it. And in that case, if it is wrong, then it is wrong, and better to make right rather than resort to an appeal to tradition (an informal fallacy, even for actually established traditions, let alone things recently added without consensus to an editing guideline). If someone had bothered to notify me eight months ago, I would have raised my objections then. Please consider an RfC in the future before adding images like these that do not actually summarize the consensus guideline. Sławomir Biały (talk) 10:41, 3 April 2017 (UTC)
- Wikipedia does not operate as a series of RfCs. If you wish to keep up with the times you will need to monitor changes just like everyone else. There was absolutely nothing controversial about how this was inserted. Carl Fredrik talk 20:12, 3 April 2017 (UTC)
- You added an image that, as far as I can tell, was not specifically discussed, and indeed was objected to at the time. The only item that you pointed to was that no one else has removed it in the relatively short time since you added it. Moreover, you added it in a sequence of edits, and did not clearly announce the change (which you should have anticipated would be controversial). Based on the current consensus, I believe that the image should be removed. You are, of course, free to establish the consensus that you claim existed by pointing to that consensus in a discussion archive, or by actually starting an RfC on the subject. Sławomir Biały (talk) 21:10, 3 April 2017 (UTC)
- What objection are you referring to that predates your current one. Please suggest improvement, if we are simply debating whether to include an image or not we are stuck at an impasse. Carl Fredrik talk 22:18, 3 April 2017 (UTC)
- It is quoted in the comment above, and includes an attribution. One editor insisting that his own image must say in a policy page, against multiple editors saying it should be removed, is not an "impasse". Generally speaking, changes like this to policy require positive consensus. I do not see evidence that this was ever sought. Sławomir Biały (talk) 22:57, 3 April 2017 (UTC)
- Two editors objecting on flawed grounds or that object only because something is not perfect hold less weight than the implicit consensus of the passage being included for 8 months. Neither is the image my own as it was created with the input and collaboration of a multitude of editors. There is no such praxis to require what you call "positive consensus" — such a phenomenon does not exist. Carl Fredrik talk 00:28, 4 April 2017 (UTC)
- The "implicit consensus" appears to have been imagined. Surely, if there were such a consensus, then other editors in support of that consensus would have made their opinions known by now. Multiple editors have here objected to the graphic, and the only commentary I could find anywhere about this graphic in the discussion archive argued against its inclusion. You are, of course, still welcome to point to any discussion that took place regarding whether this graphic was an accurate summary of the guideline, in support of your contention that some consensus was reached. But it does seem to have been sneaked in amid a flurry of edits, without any explicit discussion on your part, and as a result the implications of the graphic appear to have been largely ignored until now. Sławomir Biały (talk) 09:30, 4 April 2017 (UTC)
- Two editors objecting on flawed grounds or that object only because something is not perfect hold less weight than the implicit consensus of the passage being included for 8 months. Neither is the image my own as it was created with the input and collaboration of a multitude of editors. There is no such praxis to require what you call "positive consensus" — such a phenomenon does not exist. Carl Fredrik talk 00:28, 4 April 2017 (UTC)
- It is quoted in the comment above, and includes an attribution. One editor insisting that his own image must say in a policy page, against multiple editors saying it should be removed, is not an "impasse". Generally speaking, changes like this to policy require positive consensus. I do not see evidence that this was ever sought. Sławomir Biały (talk) 22:57, 3 April 2017 (UTC)
- What objection are you referring to that predates your current one. Please suggest improvement, if we are simply debating whether to include an image or not we are stuck at an impasse. Carl Fredrik talk 22:18, 3 April 2017 (UTC)
- You added an image that, as far as I can tell, was not specifically discussed, and indeed was objected to at the time. The only item that you pointed to was that no one else has removed it in the relatively short time since you added it. Moreover, you added it in a sequence of edits, and did not clearly announce the change (which you should have anticipated would be controversial). Based on the current consensus, I believe that the image should be removed. You are, of course, free to establish the consensus that you claim existed by pointing to that consensus in a discussion archive, or by actually starting an RfC on the subject. Sławomir Biały (talk) 21:10, 3 April 2017 (UTC)
- Wikipedia does not operate as a series of RfCs. If you wish to keep up with the times you will need to monitor changes just like everyone else. There was absolutely nothing controversial about how this was inserted. Carl Fredrik talk 20:12, 3 April 2017 (UTC)
- 3 quick points before I go to bed (will write a longer reply tomorrow):
- I'd also point out that one can critique any image that tries to explain complex phenomena. The image on referencing guidelines is also not perfect. There exist guidelines published by professional organizations that trump national guidelines as well. E.g.: a guideline published by the APA (independent) is generally regarded as more reliable than one published by the Chinese government.
- The images are not set in stone, but rather there to give a general idea of where a certain source falls on a continuum of sources. Maybe the best solution is to swap the arrows with some other form of denomination indicating a range of qualities. The same is true for crappy HTA reports, which exist and with the proliferation of HTAs are on the rise. That however does not mean that HTAs in general are not great sources, just that some aren't. Carl Fredrik talk 16:39, 2 April 2017 (UTC)
- (ec)You argue that there is a "confusion...present in the text". I don't see it. The text certainly is less absolute in its suggestions. It offers very qualified, conditional guidance about which types of sources may be more robust under some circumstances, rather than sorting them into a strict pecking order—but that's a feature, not a bug. Your diagram implies a strong – if not absolutely rigid – ranking which does not capture the much more flexible and nuanced approach that we tend to follow when evaluating sources.
- The improvement suggested, to be blunt, is to remove the misleading image. The absence of critique shouldn't be terribly surprising; you inserted it (as you have with other controversial and subsequently rejected changes) without making any comment on this talk page or engaging in any discussion. It was added as part of a flurry of more than 20 consecutive edits, large and small. Speaking for myself, I didn't even notice it had been added until today, when Sławomir Biały pointed it out and removed it. (Honestly, I expect we'll also have to have this same discussion about the "Referencing a Guideline" figure which you added in the same flurry, without so much as an edit summary: [5].) TenOfAllTrades(talk) 17:00, 2 April 2017 (UTC)
- I'm sorry, what do you mean by other controversial changes that were reverted? That is not something I am aware of, and I don't think any of those who frequent this page ave seen any such edits. I don't have time right now to explain why most of the arguments against the image here are false — but they are and I can give you the full picture soon (especially a strong refutation of the previous remarks by Slawomir immidiately above this thread). Also be aware there is considerable discussion on WT:MED, so that once discussion occurs here it is often fleeting and more of a rubber stamp. If you wish to keep up you may want to follow that talk-page, and be aware of what is tacit consent (stability over a year is more than enough to imply that). Guidelines are not static, and if you do not wish to reread them from time to time you may want to keep up with their evolution in real time. The solutions is not to go back to prior versions just because you missed the changes. Carl Fredrik talk 20:32, 2 April 2017 (UTC)
- The most significant example(s) would be from September (and then October) of last year, when you added a table that tried to summarize criteria for evaluating sources. The first time around, you added the table without any discussion; another editor (User:Jytdog) moved it to the talk page to discuss: Wikipedia talk:Identifying reliable sources (medicine)/Archive 26#Proposed MEDDUE section. A month later, you posted a modified version to the talk page to seek consensus (a good idea) but then you went ahead and added your preferred version to the article over unanimous objection on the talk page (bad) and then edit warred to try to keep it in the guideline (worse), only stopping when I told you the next step would be a review of your conduct at AN/I. TenOfAllTrades(talk) 15:22, 3 April 2017 (UTC)
- That is an extremely inaccurate summary of what happened, and entirely ignores most of the picture. Carl Fredrik talk 20:14, 3 April 2017 (UTC)
- The most significant example(s) would be from September (and then October) of last year, when you added a table that tried to summarize criteria for evaluating sources. The first time around, you added the table without any discussion; another editor (User:Jytdog) moved it to the talk page to discuss: Wikipedia talk:Identifying reliable sources (medicine)/Archive 26#Proposed MEDDUE section. A month later, you posted a modified version to the talk page to seek consensus (a good idea) but then you went ahead and added your preferred version to the article over unanimous objection on the talk page (bad) and then edit warred to try to keep it in the guideline (worse), only stopping when I told you the next step would be a review of your conduct at AN/I. TenOfAllTrades(talk) 15:22, 3 April 2017 (UTC)
- I'm sorry, what do you mean by other controversial changes that were reverted? That is not something I am aware of, and I don't think any of those who frequent this page ave seen any such edits. I don't have time right now to explain why most of the arguments against the image here are false — but they are and I can give you the full picture soon (especially a strong refutation of the previous remarks by Slawomir immidiately above this thread). Also be aware there is considerable discussion on WT:MED, so that once discussion occurs here it is often fleeting and more of a rubber stamp. If you wish to keep up you may want to follow that talk-page, and be aware of what is tacit consent (stability over a year is more than enough to imply that). Guidelines are not static, and if you do not wish to reread them from time to time you may want to keep up with their evolution in real time. The solutions is not to go back to prior versions just because you missed the changes. Carl Fredrik talk 20:32, 2 April 2017 (UTC)
I think some other editors need to weigh in, but so far I count two opposed to inclusion of the image, and one supporting it (who was also the same editor who added the image in the first place). Additionally, the above quotation from the archive appears to show that the image was not added with consensus to begin with. Ordinarily, this would count as a clear consensus against the image. Was there any place in the discussions that took place where some editor besides Carl Fredrik commented positively on this image? Sławomir Biały (talk) 10:35, 3 April 2017 (UTC)
- If the image is intended to summarise the policy it should also include timeliness. Readability of the source in my view should be less of a concern than its authoritativeness. There is always the option of adding a "lay summary" to the reference. JFW | T@lk 12:38, 3 April 2017 (UTC)
- Would a suitable correction be to change quality -> authority (in the image) and to amend the section on timeliness/weighing sources, Jfdwolff?
- We could mention that each source falls on a continuum of different factors that make it good/bad. Incidentally TenOfAllTrades, this is exactly what was proposed in October that went through a period of contention before being place on hold (mainly because I did not have time to improve it, not because of any threats). We could still pick this up and work on the following:
- Proposed MEDUE section
Any source used in a medical article is weighed on multiple axes, with: quality of the source; authority of the source; date of publishing; and relevance; all being important. Each must be taken into consideration.
| Relevance | Quality | Age | Best possible | ||||||
| Appropriate | Same topic | AND | High | AND | <2 years | OR | Yes | ⇨
|
High |
| Related topic | OR | Medium-high | OR | 2-5 years | OR | One of several | |||
| Same field | OR | Medium-low | OR | 6-9 years | OR | One of many | |||
| Inappropriate | Unrelated | OR | Low | OR | 10+ years | OR | No | ||
| Term | Unrelated | Low quality | Old | Better source available |
Amble belonging to the previous discussion that needs some rewriting to take into account a number of points raised then and now
|
|---|
Try to avoid bias when selecting sources. Bias can arise from your search criteria and search tools, and in which sources you have access to (see for example FUTON bias). |
Best, Carl Fredrik talk 20:20, 3 April 2017 (UTC)
- One alternative update:
| Relevance | Authority * | Quality * | Age | Best possible | Suitability | ||||||
| Appropriate | Same topic | AND | High | AND | High | AND | < 2 years | ⇨
|
Yes | ⇨
|
High |
| Related topic | OR | Medium-high | OR | Medium-high | OR | 2–5 years | OR | One of several | ⇨
|
Medium | |
| Same field | OR | Medium-low | OR | Medium-low | OR | 6–10 years | OR | One of many | ⇨
|
Low | |
| Inappropriate | Different field | OR | Low | OR | Low | OR | Significantly older | OR | No | ⇨
|
Unsuitable |
| Reason for rejection |
Unrelated | Low authority | Low quality | Old | Better source available |
Unsuitable | |||||
| For each source consider the lowest possible score when judging suitability. This table is not exhaustive and other factors may come into play. Whether a source is the best possible or among the best possible is the most important factor. * See text on how to judge authority and quality |
- Needs some reformatting to make it look decent
- Best, Carl Fredrik talk 20:35, 3 April 2017 (UTC)
- This is not bad. Not sure where to comment on the book graphic discussion with this now brought in. I am ambivalent about the graphic but I feel very strongly that WP:MEDRS needs to remain very stable as we would be completely fucked without it; i can't imagine the struggles that people went through while MEDRS was being built and consensus created for it. Its strength flows from the widespread consensus it holds. It is not a rulebook to be imposed -- it expresses consensus, broadly held. Do not destabilize it. Do not try to force changes into it. Jytdog (talk) 00:42, 4 April 2017 (UTC)
- Then we should not be deleting stuff that has been in there for nearly a year, just because one user opposes it. The introduction seems non-controversial, and it was in there for 8 months — if we want stability we should restore the image until consensus is achieved whether to include it or not. Anything else is in fact destabilizing. Carl Fredrik talk 00:47, 4 April 2017 (UTC)
- Am not going to rehash issues around your behavior at this guideline from last year. Jytdog (talk) 00:52, 4 April 2017 (UTC)
- Yeah, there are very different ways to look at that. Reverting based solely on the argument of no-consensus is disruptive — which is what you were doing last year. The issue is just as much about your behavior, and I don't think it is helpful to drag that into the picture, especially considering what other issues exist.
- That I hold this guideline dear and find it important to keep it current so that we aren't stuck in a status quo that permits horrible misreadings (such as the no peer-review section, with unfortunately builds upon a fundamental misunderstanding of peer-review is — hence the horrible nature of that section and the Wikilawyering it allows: because it allows us to debate what peer review is) or let poor wording hang around: does not count against anything.
- Also if anyone here were to look at the history, most of the edits on this guideline are reverts in some form, that is simply due to the nature of it — and hardly anything controversial: when most of what is being changed is done by those who have no idea what they are doing, or are trying to sneak in loopholes permitting them to reference their favorite quack-journal. What however is unusual is to remove long-standing content — thus it requires discussion, and hopefully in such a manner that it should improve the guideline in the end, not restore it to some status quo of 12 months ago. Carl Fredrik talk 01:03, 4 April 2017 (UTC)
- Carl, while considering these changes to guide book source quality, can we have a look at the pyramids in WP:MEDASSESS, perhaps with the idea of consolidating the table information above into a graphical pyramid? For MEDASSESS itself, I've thought for some time that those references are old and require the user to interpret between them. Perhaps they could be synthesized into one graphic of our making. --Zefr (talk) 01:41, 4 April 2017 (UTC)
- Am not going to rehash issues around your behavior at this guideline from last year. Jytdog (talk) 00:52, 4 April 2017 (UTC)
- Then we should not be deleting stuff that has been in there for nearly a year, just because one user opposes it. The introduction seems non-controversial, and it was in there for 8 months — if we want stability we should restore the image until consensus is achieved whether to include it or not. Anything else is in fact destabilizing. Carl Fredrik talk 00:47, 4 April 2017 (UTC)
- As an administrative note, this discussion should probably be carved into a new thread, since it seems to be only tangentially related to the now-removed image at the top of the thread. It proposes making a substantial addition to the body of MEDRS, and deserves to be presented in a way that ensures maximum exposure (and avoids the problem CFCF/Carl encountered above, where a change was introduced without discussion, and then undone when noticed months afterward.)
- That said, the proposed table is very similar to one which CFCF introduced in September/October last year, and which was roundly rejected in a discussion at the time. See Wikipedia talk:Identifying reliable sources (medicine)/Archive 26#Proposed MEDDUE section. Briefly, I see three issues.
- Much of the table is just padded with filler: extra words to fill in boxes, without helping an editor to understand or apply MEDRS. For example, it's reasonable (though not terribly helpful) to say that we prefer high-quality sources. It's pointless padding to create a four-point, color-coded scale, with scoring categories "high", "medium-high", "medium-low", and low", and no specific guidance beyond a pointer (in the explanatory notes below) to MEDASSESS. The "Authority" column has the same problem.
The "Relevance" and "Best possible" columns do little more than restate straight-up common sense. This isn't specific to MEDRS; for any claim on Wikipedia we strive to use the best possible sources which are directly relevant to the topic. - The non-'filler' content may be misleading or actively harmful. Introducing the concept of a "score" has a long and troubled history, where inexperienced editors who don't have the background to read the medical literature knowledgeably and competently instead check by rote to see if a source 'ticks all the boxes'. The issues surrounding the 5-year rule of thumb and the problems with setting out very specific age strata have been extensively criticized, including the last time around.
- If we drop the filler and the misleading stuff, the entire table is readily replaced by one sentence along the lines of "In choosing sources, we prefer high-quality, reputable, relevant, recent publications."
- Much of the table is just padded with filler: extra words to fill in boxes, without helping an editor to understand or apply MEDRS. For example, it's reasonable (though not terribly helpful) to say that we prefer high-quality sources. It's pointless padding to create a four-point, color-coded scale, with scoring categories "high", "medium-high", "medium-low", and low", and no specific guidance beyond a pointer (in the explanatory notes below) to MEDASSESS. The "Authority" column has the same problem.
- In other words, it's drawing a picture for drawing a picture's sake, while adding in some new and unhelpful concepts not actually intended to be part of MEDRS. Lest CFCF continue to mistaken silence for agreement, I will explicitly note here that I strongly disagree with the addition of this or any substantially similar table or graphic. TenOfAllTrades(talk) 14:59, 6 April 2017 (UTC)
- Just about everything you just said is wrong:
- This is highly relevant to the above discussion and has to do with the same issues that the image is meant to address. The jury is also still out on whether to include the image or make some minor changes to it. Please do not assume that things here are static or that we have now reached a consensus, we really have not.
- No, we could not replace it with a single sentence, however, we could replace it with a paragraph. But the problem there is that people don't read paragraphs of texts wedged in the middle of policy documents. MEDRS needs updating and your attitude is not helpful, and I would suggest that those who do not have at least some experience of editing medical articles not come with comments on what could be "dangerous" or not. Regarding the 5 year rule, that has been both criticized and lauded, with some of this guideline being far stronger in suggesting adherence to a 5 year cutoff. Neither does the current iteration even mention such a cutoff — it simply summarizes what consensus exists in high-level scientific literature that evidence changes over time. There are a multitude of sources for this, and I am growing ever more frustrated that editors with no experience in the field believe they can convincingly argue that there is no reason for such a cutoff. Don't make such statements without sources, and if we really want to debate it we need to go to the sources (it is a far to large discussion to be banded together with the rest of this — which is why no cutoff is included in the current iteration!)
- For the record, I strongly contest the notion that anything at all in that table is misleading. Whether some of it is a reiteration of common sense or not is beside the point. What is common sense to some is not common sense to others, and we are constantly stuck with problems where quacks try to subvert common sense with nonsense — hence: a good, easy to understand image is very, very helpful when directing new or bad faith editors to policies. Whether or not the words "medium high/medium low" need to be included is a very minor issue — the reason they are included is to indicate that a source falls along a continuum, and there are not only the high/low authority, reliability etc. levels. If there are other ways to indicate this — nothing is stopping us from using these instead — and I will reiterate: come with suggestions instead, not just "remove everything, because it isn't perfect".
- Policies aren't written for experienced Wikipedia-editors, they are written to guide those that do not have the experience to intuitively know when and where a certain rule can or should be applied. Images are not superfluous, and do not exist for their own sake — they exist because they help readers remember and get a quick overview of the contents of the text. Do not assume that everyone reads every sentence of text. The specific paragraphs of text are important when referencing them in disputes, but far more important in general editing is the jist of a guideline: the way ordinary editors understand it. And here images are extremely helpful. So unless something is actively wrong (I do not think it is, and most if not all criticism here is debunked) — there is very good reason to include images.
- There is no mistake in seeing the stability of a section over years as tacit consent.
- What is a mistake is to see minor fluctuations in which non-regular editors attend to this guideline as implication of the state of consensus over time. Carl Fredrik talk 10:33, 7 April 2017 (UTC)
- I'm not sure what qualifies as a "non-regular editor". We've both been editing Wikipedia for about as long. Is the contention that an editor who isn't carefully watching the day-to-day changes of a guideline is not a "regular editor" of Wikipedia, and therefore their opinion counts for less than a "regular editor" who (apparently) has a license to add things to guidelines without consensus? In any case, presumably the "regular editors" who supposedly form this consensus that you have repeatedly claimed have had a more than ample chance to comment here. Their silence is deafening. Sławomir Biały (talk) 12:21, 7 April 2017 (UTC)
- I believe it was clear that I was referring to regulars to this guideline page/talk page. 16:14, 7 April 2017 (UTC)
- Stated for simple analogy, MEDRS is a traffic jam for less experienced editors to navigate, and more experienced editors rely on it being clear and intuitive enough to substantiate chosen sources or reject poorly sourced statements. Tables and graphics can be to MEDRS as highway and intersection signs are to traffic. There is abundant text for more detailed guidance. I support the clarity and immediate visual interpretation that color graphics can offer. --Zefr (talk) 15:11, 7 April 2017 (UTC)
- An excellent analogy, that captures my feelings towards the guideline entirely. Carl Fredrik talk 16:14, 7 April 2017 (UTC)
- I'm not sure what qualifies as a "non-regular editor". We've both been editing Wikipedia for about as long. Is the contention that an editor who isn't carefully watching the day-to-day changes of a guideline is not a "regular editor" of Wikipedia, and therefore their opinion counts for less than a "regular editor" who (apparently) has a license to add things to guidelines without consensus? In any case, presumably the "regular editors" who supposedly form this consensus that you have repeatedly claimed have had a more than ample chance to comment here. Their silence is deafening. Sławomir Biały (talk) 12:21, 7 April 2017 (UTC)
Mismatch
"Supplemental Vitamin E and selenium can increase the risk of prostate cancer." (citing PMID 23552052)
This example sentence does not match the results/discussion of selenium in the cited source (per conclusions here).
Given the nuanced discussion of the (inconclusive) findings for selenium, perhaps better to restrict the example to Vitamin E. 86.186.155.183 (talk) 08:37, 13 June 2017 (UTC)
- Another (basic) conceptual mismatch fixed here (see PMID 20924966). 86.186.155.183 (talk) 10:07, 13 June 2017 (UTC)
- Thanks. fixed further. Jytdog (talk) 15:28, 13 June 2017 (UTC)
Edit request
This edit request to Wikipedia:Identifying reliable sources (medicine) has been answered. Set the |answered= or |ans= parameter to no to reactivate your request. |
Maybe someone qualified would be able to fix the paragraph about health technology assessments that follows the section on medical and scientific organizations. You could add an asterisk after some British organization who claims the orphan, or omit the paragraph. Thank you. -SusanLesch (talk) 19:17, 3 July 2017 (UTC)
 Not done That page is not protected and does not require an administrator to update. — xaosflux Talk 20:16, 3 July 2017 (UTC)
Not done That page is not protected and does not require an administrator to update. — xaosflux Talk 20:16, 3 July 2017 (UTC)
- Hi, Xaosflux. Correct. However we need a qualified editor with knowledge of the UK health system to make the edit. Pardon me for choosing a template that Wikipedia has. -SusanLesch (talk) 23:04, 3 July 2017 (UTC)
- I have to admit I do not understand your request either. Carl Fredrik talk 23:35, 3 July 2017 (UTC)
- First, sorry, @Xaosflux: I imagine that template set off an alarm somewhere that you answered! Second, CFCF. What don't you understand? The guidelines have an orphan asterisked section referring to nothing that needs attention. -SusanLesch (talk) 23:41, 3 July 2017 (UTC)
- See the image. It has nothing to do with the UK. Carl Fredrik talk 00:09, 4 July 2017 (UTC)
- Thank you, @CFCF: I missed that HTA! I leave it to you guys to decide if it makes more sense as part of the caption. (I don't think we have HTAs in the U.S. but maybe we do!) -SusanLesch (talk) 00:14, 4 July 2017 (UTC)
- See the image. It has nothing to do with the UK. Carl Fredrik talk 00:09, 4 July 2017 (UTC)
- First, sorry, @Xaosflux: I imagine that template set off an alarm somewhere that you answered! Second, CFCF. What don't you understand? The guidelines have an orphan asterisked section referring to nothing that needs attention. -SusanLesch (talk) 23:41, 3 July 2017 (UTC)
- I have to admit I do not understand your request either. Carl Fredrik talk 23:35, 3 July 2017 (UTC)
- Hi, Xaosflux. Correct. However we need a qualified editor with knowledge of the UK health system to make the edit. Pardon me for choosing a template that Wikipedia has. -SusanLesch (talk) 23:04, 3 July 2017 (UTC)
- @SusanLesch: yes, we have a few of those - ensuring that protection does not get in the way of edits that improve the project is an import task for admins. — xaosflux Talk 00:22, 4 July 2017 (UTC)
- @Xaosflux: thank you for being an emergency responder. I will try not to send a false alarm ever again
 Also I learned that the World Health Organization thinks the United States does have HTAs. -SusanLesch (talk) 14:05, 4 July 2017 (UTC)
Also I learned that the World Health Organization thinks the United States does have HTAs. -SusanLesch (talk) 14:05, 4 July 2017 (UTC)
- @SusanLesch: never worry about that - I'd rather there be a bunch of false positives then block helpful edits! — xaosflux Talk 14:09, 4 July 2017 (UTC)
- @Xaosflux: thank you for being an emergency responder. I will try not to send a false alarm ever again
Medical source for non-medical claims
One editor claims a medical source cannot be used for a non-medical claim. I thought reviews can be used for non-medical claims. QuackGuru (talk) 23:20, 14 August 2017 (UTC)
- I get the feeling that this would depend very much on the specifics. But as long as the medical review directly addresses that non-medical claim, I cannot see any basis in policy or guidelines to indicate that it would be an inappropriate source. If medical and non-medical sources differ in what they say about the claim, then there would be matters of due weight to consider. --Tryptofish (talk) 23:25, 14 August 2017 (UTC)
- MEDRS requires medical sources for medical claims. RS does not require nonmedical sources for nonmedical claims. Seppi333 (Insert 2¢) 23:26, 14 August 2017 (UTC)
- Yes indeed. But I'm wondering: if the medical source covers the claim, would that claim really be non-medical, because if it were really non-medical, why would the medical source be talking about it? --Tryptofish (talk) 23:30, 14 August 2017 (UTC)
- It is for non-controversial facts. I think it should be mentioned in MEDRS that medical sources or reviews are reliable for non-medical claims. QuackGuru (talk) 23:31, 14 August 2017 (UTC)
- If medical and non-medical sources say the same thing about it, as being noncontroversial, then it seems like a moot point. As Seppi333 said, it becomes a matter of WP:RS. --Tryptofish (talk) 23:35, 14 August 2017 (UTC)
- I have not checked if non-medical sources say anything about it. I could not find where WP:RS mentions using medical sources for non-medical claims. QuackGuru (talk) 23:41, 14 August 2017 (UTC)
- To clarify what I meant to say, the absence of anything in RS saying not to cite it should mean that it's not a problem. There can be issues of WP:CREEP in spelling these things out. I think that it would be enough to ask the editor who objects to the citation to provide a guideline that says that it should not be cited. --Tryptofish (talk) 23:50, 14 August 2017 (UTC)
- I won't be asking an editor who is mass deleting content. QuackGuru (talk) 23:54, 14 August 2017 (UTC)
- To clarify what I meant to say, the absence of anything in RS saying not to cite it should mean that it's not a problem. There can be issues of WP:CREEP in spelling these things out. I think that it would be enough to ask the editor who objects to the citation to provide a guideline that says that it should not be cited. --Tryptofish (talk) 23:50, 14 August 2017 (UTC)
- I have not checked if non-medical sources say anything about it. I could not find where WP:RS mentions using medical sources for non-medical claims. QuackGuru (talk) 23:41, 14 August 2017 (UTC)
- If medical and non-medical sources say the same thing about it, as being noncontroversial, then it seems like a moot point. As Seppi333 said, it becomes a matter of WP:RS. --Tryptofish (talk) 23:35, 14 August 2017 (UTC)
- It is for non-controversial facts. I think it should be mentioned in MEDRS that medical sources or reviews are reliable for non-medical claims. QuackGuru (talk) 23:31, 14 August 2017 (UTC)
- Yes indeed. But I'm wondering: if the medical source covers the claim, would that claim really be non-medical, because if it were really non-medical, why would the medical source be talking about it? --Tryptofish (talk) 23:30, 14 August 2017 (UTC)
Discussion moved. See Wikipedia talk:Identifying reliable sources#Medical source for non-medical claims. QuackGuru (talk) 23:54, 14 August 2017 (UTC)
Should WP:MEDRS be applied to ethnobotany?
I've recently extended the article about the plant Pentadiplandra, including an extensive account of its applications in traditional medicine. This is admittedly generally quite old information that was gathered by plant collectors around the location the plant was found, along with e.g. local names. This information does not state wether the different preparations actually are effective or not, but generally reflect the understanding of the collectors about which (combination of) plant(s) was prepared, in what way it was applied, in case of which ailment, and by which people or in which area. Of cause we need to take care the reader is not misled to think this implies the preparations are really working. One of our colleagues removed almost all of that information, leaving a few statements, having several citations each and putting an "inadequately cited" template above the section. Is there any consensus that ethnobotanic information should be subject to WP:MEDRS? Dwergenpaartje (talk) 17:26, 7 August 2017 (UTC)
- Yup high quality sources like major textbooks should be used. Doc James (talk · contribs · email) 17:30, 7 August 2017 (UTC)
- Well... in my view, if the traditional medicinal uses are described as a cultural practice and named as traditional medicine then I think this goes in Society and culture and regular old RS are OK. If it is stated as an actual health practice and put under a header like "Health effects" then MEDRS are needed. Now I go look and see what was done... Jytdog (talk) 17:34, 7 August 2017 (UTC)
- I looked at this version and most of those uses were completely unsourced (not just a MEDRS issue) and were appropriately removed in these diffs by Zefr. I tweaked it a bit more. Jytdog (talk) 18:27, 7 August 2017 (UTC)
- I agree with Jytdog that MEDRS are needed for anything concerning health effects, but not needed for the cultural basis. Similarly, for example, in pages about diseases, we apply MEDRS for all of the actual health-related issues, but there is no need for MEDRS when discussing the history. In content about "the plague", use MEDRS for clinical treatment, but there's no need for MEDRS for what happened in Europe centuries ago. Same concept for ethnobotany. --Tryptofish (talk) 18:38, 7 August 2017 (UTC)
- I too agree with Jytdog; part of the issue with the original was the balance of the article. Too high a proportion of a plant article on traditional medical uses can create a false impression of its medical value. By the way, there is a template for plant articles; traditional medicine goes in the Uses section. Peter coxhead (talk) 18:50, 7 August 2017 (UTC)
- ah! there is always stuff i don't know. "traditional uses" under uses makes sense, and doesn't need MEDRS there. Jytdog (talk) 21:06, 7 August 2017 (UTC)
- User:Jytdog, in the version you had a look at, every statement is covered by the references sources. However, the referencing was not done for each statement individually. I've now seen that some editors specify in non-wiki which statements are covered by a specific reference, and I will copy that approach whenever I think debate might arise.
- Concerning our discussion here, I think it would be useful to have a short section on WP:MEDRS on etnobotanical information. Perhaps it could read something along the following lines: "Ethnobotanical information - how plants are, or used to be, applied by indigenous people - should not be included in the Medicine subsection, but rather in a Traditional medicine subsection. As anywhere on Wikipedia, tertiary and secondary sources are preferable to primary sources, but primary sources for ethnobotanical information are certainly allowable. Care has to be taken however, that efficacy of these tradional uses is not inadvertendly suggested, such as by extensive listing of comparable uses, by excessive referencing, by weaving in primary research into the efficacy of such plant preparations, or by having a long sections compared to the rest of the article. Any information on the health effects needs to adhere to WP:MEDRS, even if it would be included under a different heading than Medicine." Dwergenpaartje (talk) 12:59, 8 August 2017 (UTC)
- I agree that it would be good to include something explicit on how to handle traditional medical uses of plants (ethnobotany is wider, covering all traditional uses of plants, such as for food, fibre, building, etc.). It's a constant source of editing disputes concerning plant articles. It could either be put at WP:PLANTS/Template and cross-referenced from WP:MEDRS or vice versa. Peter coxhead (talk) 13:10, 8 August 2017 (UTC)
- I agree with this proposal. For the article on Dermatitis, I was suggesting a section on ethnopharmacy after AGF edits by an IP which added unsourced Chinese herbs into one of the sections. Inclusion in pharmacopoeia, which indicate standardisation of a plant preparation in the specific country the publication was made for, is usually done for local herbal remedies that have been approved by the country's Food and Drug Administration for homogenisation of dosage form, not necessarily therapeutic claims. Apart from these, ethnopharmacological studies done on the plant in question may also serve as a more valid reference for their inclusion into such a category. --a u t a c o i d (stalk) 01:57, 22 August 2017 (UTC)
- ah! there is always stuff i don't know. "traditional uses" under uses makes sense, and doesn't need MEDRS there. Jytdog (talk) 21:06, 7 August 2017 (UTC)
WP:MEDRS is based on a sham
WP:MEDRS is based on lousy references. Not WP:reliable sources.
- Big Pharma Is America’s New Mafia. From the article:
| In fact, the heavy influence of pharmaceutical dollars inspired the former editor-in-chief of the New England Journal of Medicine, Dr. Marcia Angell, to conclude, “It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines.” |
--Timeshifter (talk) 10:38, 31 July 2017 (UTC)
- Proposal - All those who like WP:MEDRS despite its perceived flaws, please iVote "I Like It" -Roxy the dog. bark 10:43, 31 July 2017 (UTC)
- I Like It, as nom. -Roxy the dog. bark 10:43, 31 July 2017 (UTC)
Let's try addressing the issue instead. --Timeshifter (talk) 13:11, 31 July 2017 (UTC)
- What issue? -Roxy the dog. bark 14:12, 31 July 2017 (UTC)
- We try to use the best available sources, those that impart current accepted medical knowledge. This doesn't mean the sources are always right, but in principle they are least likely to be wrong. By definition, using anything less than the best available sources is suboptimal. Sizeofint (talk) 15:16, 31 July 2017 (UTC)
- @Timeshifter:, what words in the guideline are you suggesting we change, and to what? LeadSongDog come howl! 15:25, 31 July 2017 (UTC)
- Timeshifter, you have just become aware of Angell? Welcome to the party. Many of us have been aware of what she says for a long time. You should actually read MEDRS; like RS it calls us to use secondary sources. The sources Angell has criticized are primary sources under this guideline and we rarely use them and when we do it is with great care (just like RS says... perhaps more strictly here). And as LeadSongDog says, you are in any case not making a concrete proposal.Jytdog (talk) 15:55, 31 July 2017 (UTC)
- Yup MEDRS is excellent. It is a guideline on how to write WP's medical content. It is an internal document not a forward facing medical article and therefore does not need to be based on MEDRS sources. Doc James (talk · contribs · email) 16:12, 31 July 2017 (UTC)
- The quality of a significant proportion of "respectable" medical research is indeed troubling. MEDRS is the best available guide on how to use it. I suppose nothing is perfect; what changes to MEDRS would you suggest? Richard Keatinge (talk) 17:05, 31 July 2017 (UTC)
- That section header sure did get my attention! There is, indeed, a deep-rooted problem with primary research at a time when investigators are often desperate to keep their jobs (and it actually has very little to do with Big Pharma). But one thing that MEDRS does very well is that it emphasizes the use of review articles instead of primary sources, which tends to filter out primary sources that do not get reproduced. (This discussion reminds me of the long-ago discussions about "verifiability, not truth": Wikipedia can cite sources, and try hard to rely only on good sources, but we cannot vouch for sources' accuracy.) --Tryptofish (talk) 00:38, 1 August 2017 (UTC)
Review articles are based on primary articles. Crap mixed well is still crap. WP:NPOV means that all significant viewpoints must be represented. WP:MEDRS is used to block WP:NPOV. The Review Overlords block opposing points of view. The WP:MEDRS exception to the guidelines. --Timeshifter (talk) 01:23, 1 August 2017 (UTC)
- I will not be responding here further. Jytdog (talk) 01:26, 1 August 2017 (UTC)
Concerning reviews, here below is part of this thread: Wikipedia talk:WikiProject Medicine/Archive 100#Saturated fat and cardiovascular disease controversy:
|
At least in that area there are many reviews, and so no one review is used to squash all other significant viewpoints. See WP:NPOV. But in many health articles on Wikipedia, there is One Review To Rule Them All. More recent info is blocked no matter the source. Gold-standard epidemiological studies, be damned. --Timeshifter (talk) 21:50, 1 August 2017 (UTC)
- I'll make a last reply here. Wikipedia runs on consensus. To gain consensus you have to persuade people, and make reasonable arguments about making reasonable changes, and it takes a good long while to get really broad and deep consensus.
- If you really want to improve WP and move MEDRS in a direction that you think would lead to stronger content throughout WP, I suggest you think about how to move MEDRS in that direction, incrementally. That would mean offering a concrete proposal, and persuading people through careful discussion.
- I ~think~ you are probably well-intentioned but from your section header on down, you have set yourself up to fail to persuade anybody. Too much of this is angry sledgehammer - you are just banging your head against the wall doing it this way. Jytdog (talk) 22:17, 1 August 2017 (UTC)
- Saying that this guideline is based on "lousy references" shows a complete misunderstanding of its purpose. MEDRS is a guideline that promotes a hierarchy of evidence. Unfortunately even reviews come at varying levels of quality, and it is not unusual for otherwise good quality secondary sources to promulgate discredited concepts. Editorial judgement and consensus are ultimately the real arbiters.
- As Jytdog said, please identify specific areas of this guideline that you believe should be revised. The guideline itself is supported by a broad platform of editors so there's not much point trying to discredit it as a whole based on your personal perceptions of its utility. JFW | T@lk 22:36, 1 August 2017 (UTC)
The problem is deep at so many levels. Systemic bias is a big problem with WP:MEDRS. Who reviews the reviewers? Whose money funds them? Whose money funds the initial studies? Whose money funds the text books? Whose money pays for the ads in peer-reviewed medical journals? How is Wikipedia reviewing the quality of medical journals used as references? Per the comments of Dr. Marcia Angell, the former editor-in-chief of the New England Journal of Medicine. She says that much at all 3 levels (clinical research, trusted physicians, authoritative medical guidelines) can not be believed. So that means Wikipedia has to look at how much has been proven questionable over time. And why. In-depth analysis of each medical journal and reviewer by Wikipedia to determine how often they have not been reliable: WP:RS. There is a big problem with replication of studies due to the fact that Big Pharma can pay a lot more for clinical studies than naturopaths. Due to the money made on pharmaceutical patents. Chemicals found in nature, many nutraceuticals, or anything related to diet can not be patented in nearly all cases. --Timeshifter (talk) 00:20, 22 August 2017 (UTC)
- From the tone of your comment, you seem to be promoting an appeal to nature-based guideline, which is a fundamentally flawed viewpoint. Medical research isn't perfect, especially at the primary level. We acknowledge this, and it's why WP:MEDRS exists in the first place. In a nutshell, be as far to the left as you can be on this chart.
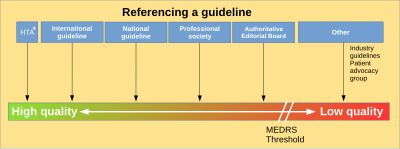
- Does this mean everything said will actually be true? No, all science is tentative. Hence WP:VNT.
- Unless you have a concrete proposal, with specifics, to improve that general guideline, you're not doing much other than screaming in the wind. Headbomb {t · c · p · b} 00:56, 22 August 2017 (UTC)
- Timeshifter, of course the problem is very deep per comments by Dr. Marcia Angell, the former editor-in-chief of the New England Journal of Medicine. But the problem is much worse if we don't follow MEDRS. Many times sources have bias. They often disagree. We often include both views and let the reader decide. Who reviews the reviewers? On Wikipedia, editors review and summarise the content. Reviews often state their COIs. Some reviews have no impact factor. They are a mixed bag. Some are excluded. It is a case-by-case basis. Is there a particular article that is a current problem? QuackGuru (talk) 01:23, 22 August 2017 (UTC)

Reviews don't seem to be peer reviewed in many cases. And the influence of money is a systemic bias, and an obstacle to getting all significant viewpoints and results: WP:NPOV. My points go beyond an appeal to nature. I am talking about an appeal to dollars. As in seeking grants for studies. As in modifying the setup, carrying out, and conclusions of studies and reviews (even slightly) to satisfy the study funders, medical journal advertisers and owners, tenure reviewers, etc.. These systemic biases effect results at all levels, and between competing patented products, not just between patented products and natural products, or diet. There are no easy solutions, and I am open to suggestions. --Timeshifter (talk) 01:28, 22 August 2017 (UTC)
- Money does influence article content because they were paid to write that review. An obstacle I encountered on Wikipedia was when an editor mass deleted reviews because they had a COI. The content was non-controversial. Deleting the reviews just because they were paid to write a review made a mess of the article. There will always be obstacles to getting all neutral viewpoints covered. They write the conclusions for the reviews and editors report what they said. It is human nature. If one author writes many reviews on a topic that can change the POV of an article. Even one detailed review can change the POV of an article. Another way for an author to get more content in Wikipedia is for the article to be in the public domain or be compatible with Wikipedia's Creative Commons. See {{PD-notice}} and see {{CC-notice}}. If the content is free to copy why not? The bigger issue for me is editors add too much detail or go in the opposite direction and delete way too much content. This often happens on controversial topics. Many articles can have misleading content. If there are a lot of reviews on a topic there is more chance all viewpoints will be covered. Writing lede for articles is sometimes tricky to write.
- See WP:MEDBIAS: "Because of this: obvious or overt bias in a source is a difficult problem for Wikipedia." Bias is common. That's the way it is. But there is a lot of content that is mundane claims where there is no disputes. Editors on Wikipedia are the filter for the content. I was reading about the fat controversy. First they told people saturated fat was bad. Now I have seen a few sources claiming it is okay in moderate. QuackGuru (talk) 02:02, 22 August 2017 (UTC)
How to use a medical source for medical claims
Editors have claimed the only the conclusion from the review may be summarized. Editors have also claimed because the review is mainly about one specific topic other points the review made are not reliable. Where does Identifying reliable sources (medicine) address this? QuackGuru (talk) 14:56, 15 August 2017 (UTC)
- Who is this editor making these absurd claims? Seppi333 (Insert 2¢) 21:55, 15 August 2017 (UTC)
- This has popped up more than once on different articles. This time it happened about two weeks ago. Another editor claims a medical source is unreliable for non-medical content. I tried adding "A MEDRS-compliant source is not inherently unreliable for non-medical content."[7] One editor replaced sourced content with original research. Then another editor deleted the content rather than revert. Then, I tried adding Material that fails verification may also be replaced with content that passes verification.[8] Policy and guidelines are not keeping up with these issues. QuackGuru (talk) 23:08, 15 August 2017 (UTC)
- Those appear to be disagreements about whether or not to specify such information on policy and guideline pages, rather than disagreements about editing a mainspace page. I'm pretty sure that Seppi333's question was about the latter, and I have the same question. --Tryptofish (talk) 23:28, 15 August 2017 (UTC)
- I'm seeing at WT:V and WP:RS that editors are disagreeing with you about these things, and not on the basis of absurd claims, but on the basis of how policy should be formulated. Please do not try to get consensus here for what you cannot get consensus there. --Tryptofish (talk) 23:33, 15 August 2017 (UTC)
- This has popped up more than once on different articles. This time it happened about two weeks ago. Another editor claims a medical source is unreliable for non-medical content. I tried adding "A MEDRS-compliant source is not inherently unreliable for non-medical content."[7] One editor replaced sourced content with original research. Then another editor deleted the content rather than revert. Then, I tried adding Material that fails verification may also be replaced with content that passes verification.[8] Policy and guidelines are not keeping up with these issues. QuackGuru (talk) 23:08, 15 August 2017 (UTC)
See WP:NOABSTRACT. I think it can be expanded. "Content other than the conclusion may also have useful content. A source that is mainly about one specific topic may have other useful content." QuackGuru (talk) 02:00, 16 August 2017 (UTC)
- Just who are all these "editors" who make these claims? Here and at WT:RS you've repeatedly rejected requests to provide any diffs or links to discussions where these purported disputes have occurred. Policy and guidelines are 'not keeping up with' problems that only you seem to encounter, but which you refuse to bring to WP:RSN, WP:AN/I, or any other noticeboard. TenOfAllTrades(talk) 03:39, 16 August 2017 (UTC)
- I can handle the socks and others. I made very good proposals across policy and guidelines to help future editors. This page is for Identifying reliable sources (medicine). QuackGuru (talk) 14:57, 16 August 2017 (UTC)
- @TenOfAllTrades: I strongly suspect this and the other 2 RS related discussions relate at least in part to the dispute Talk:Electronic cigarette/Archive 31#Represent consensus on relative safety since I'm seeing a lot of similar comments used by QG there. E.g. "A paper may be mainly about one thing, but there could be other things there are also relevant." Nil Einne (talk) 17:25, 22 August 2017 (UTC)
- Ah, I see now. That makes sense, unfortunately. TenOfAllTrades(talk) 20:27, 22 August 2017 (UTC)
New proposal
- Support. Don't just cite the conclusion: See "There may be more useful content to summarize than just the conclusion. A source that is mainly about one specific topic may have other useful content."[9] QuackGuru (talk) 14:57, 16 August 2017 (UTC)
- No need to spell out the obvious.....again !--Moxy (talk) 17:24, 16 August 2017 (UTC)
- I agree with Moxy – and pretty much everyone else who is advising that these proposals are not needed. Please understand that I am not trying to shut down discussion, but it seems to me that this has become an awful lot of discussion about things that will never get consensus. --Tryptofish (talk) 17:40, 16 August 2017 (UTC)
- First... I don't think the proposed text belongs in the section where QuackGuru proposes to place it (I am not at all clear about how it relates to the rest of the sub-section - which is about abstracts)? Second... given that QuackGuru has (repeatedly) been asked for examples of the problem, and has (repeatedly) refused to give any, I can only assume that there is not actually a problem that needs to be resolved. And given this, the proposed text is unnecessary instruction, that will likely cause more confusion than it will resolve. Finally, I too am concerned about the amount of discussion about this... in multiple venues. Disruptive forum shopping is not the way to improve the project. Blueboar (talk) 17:44, 16 August 2017 (UTC)
- You said "Finally, I too am concerned about the amount of discussion about this... in multiple venues. Disruptive forum shopping is not the way to improve the project." I did not make this specific proposal to another page. There is no other medical guideline for this content. Why would you call it disruptive forum shopping? Editors already summarise content that is not strictly from the conclusion. This is in line with what most editors are currently doing. I have seen different editors on different articles claiming only the conclusion can be summarized. It would saved time if the guideline clarifies this for future disputes. QuackGuru (talk) 01:23, 22 August 2017 (UTC)
- Comment: After waiting to weigh in, I'm going to go with Moxy on this one. Flyer22 Reborn (talk) 20:46, 22 August 2017 (UTC)
A source that is mainly about one specific topic may have other useful content
- IMO in wikipedia the term "useful content" applies to WP:NOT/WP:RELEVANCE/WP:DUE, i.e., whether a particular content is (a) encyclopedic and (b) fits the subject of a particular article. IMO in the context of our discussion, the proper term would be "usable content" (content from elsewhere which may be used in wikipedia). If this is what was in mind, then the answer is clear: the usability of content published elsewhere belongs to WP:RS rules, not here. Staszek Lem (talk) 18:41, 7 September 2017 (UTC)
Question
The guidelines describes the inclusion of recognised standard textbooks. I use textbooks all the time for references. Who decides what is 'recognized'? Can one editor 'recognize' a textbook and another not 'recognize' a textbook? Often, other books are used as textbooks and are assigned by clinical instructors. Does this make it a 'standard text book'. Amazon rents textbooks so they must have a system that identifies textbooks - which suggests that the books that are rented as textbooks. I don't want Amazon to determine what a textbook is. I apologize if this discussion has already taken place but I didn't find it. I would like to see the word 'standard' removed from the place that it appears in the phrase 'recognized textbook' because it is redundant. Best Regards, Barbara (WVS) ✐ ✉ 10:27, 22 September 2017 (UTC)
- The problem comes from certain alternative medicine books which purport to be textbooks. I don't think anyone is suggesting we should use Amazon's definition either, because for example they state that this is a textbook The Migrain Miracle... The guideline is deliberately vague, and I'm not sure this would improve it. Carl Fredrik talk 13:27, 22 September 2017 (UTC)
Books on breastfeeding
Would the following books be considered reliable sources? 1) Dr. Jack Newman's Guide To Breastfeeding, Revised Edition and 2) The Womanly Art of Breastfeeding ? Clayoquot (talk | contribs) 05:59, 24 October 2017 (UTC)
- I would say so, yes. Bondegezou (talk) 09:34, 24 October 2017 (UTC)
- A book from a celebrity doctor and one from an advocacy organisation? I'd run a mile, especially for any health assertions - which is not to say the books are wrong, but we should be supporting anything weighty with much stronger sources, and biomedical content needs WP:MEDRS. Alexbrn (talk) 09:55, 24 October 2017 (UTC)
- Why do you say that Jack Newman is a celebrity doctor? I am very surprised to hear that assertion. As for books published under the brand of an advocacy organization, would you say the same for books published by the American Diabetes Association? There seems to be a big grey area in this guideline between books published by academic and medical publishers, and self-published junk. I'd like to see more discussion and clarification on these types of books. Clayoquot (talk | contribs) 19:29, 24 October 2017 (UTC)
- Yes, we avoid patient advocacy groups of all kinds for medical assertions. A doctor appearing on a book jacket as "Dr Jack" is a celebrity doctor. And he's a known advocate also, see: Jack Newman (doctor). Looking at the book a big drum is getting a good beating! There is no dearth of sources on this topic so why consider these ones? What is it that needs to be sourced? Alexbrn (talk) 19:34, 24 October 2017 (UTC)
- Let me make sure I understand you: The jacket of the book in question has a picture of a mother and a baby, neither of whom is Jack Newman. The phrase "Dr. Jack Newman" appears twice on the cover, once in the list of authors and once in the title. And that, along with the fact that he advocates breastfeeding, makes him a celebrity doctor? And you think we should avoid, for instance, the ADA's 2017 Standards of Medical Care in Diabetes for medical assertions? Clayoquot (talk | contribs) 20:09, 24 October 2017 (UTC)
- In WP:MEDRS authors generally do not get billed as "Dr X"; this is doctor-as-brand stuff. And I repeat: we avoid patient advocacy groups of all kinds for medical assertions. In any event these books just aren't WP:MEDRS. They may be usable for sourcing mundane facts - but you haven't said what content is in question. Sources are only "reliable" (or not) in respect of content. What is the content? Alexbrn (talk) 20:24, 24 October 2017 (UTC)
- (ec) The proper venue for such discussions is WP:RSN
- Standards of care properly sourced per MEDRS should be fine. The books aren't such sources. --Ronz (talk) 20:28, 24 October 2017 (UTC)
- @Ronz:, I don't understand what you are trying to say. Are you saying that 2017 Standards of Medical Care in Diabetes is a MEDRS-compliant source because it is a "standards of care" book even though its publisher is a patient advocacy group? Or are you saying that this book is not a MEDRS-compliant source? 03:47, 28 October 2017 (UTC)
- In WP:MEDRS authors generally do not get billed as "Dr X"; this is doctor-as-brand stuff. And I repeat: we avoid patient advocacy groups of all kinds for medical assertions. In any event these books just aren't WP:MEDRS. They may be usable for sourcing mundane facts - but you haven't said what content is in question. Sources are only "reliable" (or not) in respect of content. What is the content? Alexbrn (talk) 20:24, 24 October 2017 (UTC)
- Let me make sure I understand you: The jacket of the book in question has a picture of a mother and a baby, neither of whom is Jack Newman. The phrase "Dr. Jack Newman" appears twice on the cover, once in the list of authors and once in the title. And that, along with the fact that he advocates breastfeeding, makes him a celebrity doctor? And you think we should avoid, for instance, the ADA's 2017 Standards of Medical Care in Diabetes for medical assertions? Clayoquot (talk | contribs) 20:09, 24 October 2017 (UTC)
- Yes, we avoid patient advocacy groups of all kinds for medical assertions. A doctor appearing on a book jacket as "Dr Jack" is a celebrity doctor. And he's a known advocate also, see: Jack Newman (doctor). Looking at the book a big drum is getting a good beating! There is no dearth of sources on this topic so why consider these ones? What is it that needs to be sourced? Alexbrn (talk) 19:34, 24 October 2017 (UTC)
- Why do you say that Jack Newman is a celebrity doctor? I am very surprised to hear that assertion. As for books published under the brand of an advocacy organization, would you say the same for books published by the American Diabetes Association? There seems to be a big grey area in this guideline between books published by academic and medical publishers, and self-published junk. I'd like to see more discussion and clarification on these types of books. Clayoquot (talk | contribs) 19:29, 24 October 2017 (UTC)
There are many reliable sources on breastfeeding. QuackGuru (talk) 20:46, 24 October 2017 (UTC)
- See edit history on this topic. --Zefr (talk) 23:29, 24 October 2017 (UTC)
- Neither of these books has come up in the history of the Fenugreek article, and there is no controversy in the Fenugreek article about what sources to use for information on breastfeeding. I think Zefr might have noticed that I have made edits to both the Fenugreek article and this talk page and assumed that they were related. Thanks everyone for commenting. W.r.t. the two books I asked about, let me make sure I need them and I'll inquire at WP:RSN if I need to. Clayoquot (talk | contribs) 00:17, 25 October 2017 (UTC)
Ah well, on fenugreek supplementation for breast feeding we're citing PMID 27999511, which is a better source; PMID 23468043 would be better. Alexbrn (talk) 02:46, 25 October 2017 (UTC)
- There are many practical or day-to-day issues with breastfeeding etc. that are recognised not to be well covered by the medical journal literature. I think there is a danger in treating an article on breastfeeding in exactly the same way as, say, bisoprolol. And just because a book is published for a non-professional audience does not mean that it is self-published junk or celebrity nonsense. Bondegezou (talk) 13:44, 26 October 2017 (UTC)
- If the content is biomedical and there are no MEDRS refs then we don't talk about it. If is practical stuff, like bras useful for people who breastfeed, that is not biomedical and doesn't need MEDRS. Jytdog (talk) 20:35, 26 October 2017 (UTC)
Please keep an eye on the article invaded by medical spammers. Staszek Lem (talk) 18:17, 27 October 2017 (UTC)
P.S. I would also question the notability of the subject. Staszek Lem (talk) 18:18, 27 October 2017 (UTC)
- Protected. THe question remains regarding if it should be merged. Doc James (talk · contribs · email) 19:32, 28 October 2017 (UTC)
Formatting citations
Hi. I wonder if it is possible to get the link fixed to "Formatting citations" under Biomedical journals. Thank you. -SusanLesch (talk) 23:32, 10 November 2017 (UTC)
- I think it got moved to WP:MEDMOS. --122.108.141.214 (talk) 05:41, 11 November 2017 (UTC)
- Thank you! Do you think that "If you are citing a source along with an expert summary, it is helpful to list them together, with the main source first to indicate that it is more authoritative. For example:..." was just dropped? Anyway thank you for fixing the link and for the link to 2010. -SusanLesch (talk) 15:04, 11 November 2017 (UTC)
- You're welcome. I don't use the lay summary so much, so it might be better to check with the main WT:MED page to see what everyone thinks. --122.108.141.214 (talk) 00:54, 12 November 2017 (UTC)
FTC Halts the Deceptive Practices of Academic Journal Publishers
FTC Halts the Deceptive Practices of Academic Journal Publishers. November 22, 2017. Federal Trade Commission.
Almost no one ever answers my questions about why the many sheep editing according to WP:MEDRS rules so blindly believe a review over the results of peer-reviewed studies. It is a mechanism of authority overriding normal WP:NPOV rule of showing all significant viewpoints.
I don't see peer review of reviews in many cases. Or the peer review is cursory and shallow. People endorsing the party line over the results of actual studies. --Timeshifter (talk) 21:18, 26 November 2017 (UTC)
Kirtan Kriya meditation research by Dharma Singh Khalsa
I removed what appears to be a very questionable claim of the benefits of Kirtan Kriya meditation based upon a study by Dharma Singh Khalsa, "Other forms of meditation such as Kirtan Kriya (KK), is proven to be an effective prevention method of Alzheimer's disease. This practice is proven to improve sleep, decrease depression, reduce anxiety, down regulate inflammatory genes, upregulate immune system genes and increase telomerase by 43%..." [1]
I started a discussion at Talk:Meditation#Kirtan_Kriya_content_moved_to_talk.
References
- ^ Khalsa, D. S. 2015. Stress, Meditation, and Alzheimer’s Disease Prevention: Where The Evidence Stands. Journal of Alzheimers Disease 48, 1–12.
Source type vs clinical phases
If I understand correctly primary sources should refrain. But does that mean that you must wait till later phases of clinical phases such as phase III before it is possible to write about the drug in question? Or that the drug must be approve commercially? — Preceding unsigned comment added by 2001:4642:B111:0:C5A8:F00C:7A7:57FB (talk) 18:57, 20 January 2018 (UTC)
- Whether there are MEDRS sources is independent of the clinical stage. It is true that the further along a drug candidate is, the more likely it will be, to be discussed in a MEDRS source. But not always. One just has to look. Everything in Wikipedia arises from sources... you start there, not with the development status of the compound. Does that make sense? Jytdog (talk) 19:36, 20 January 2018 (UTC)
MEDDATE
This is being discussed in part at Wikipedia_talk:WikiProject_Medicine#Deleting_Cochrane_Reviews_more_than_10_yrs_old?. But the addition of "often" isn't very useful in my view. Adding that isn't horrible, but it doesn't really fix or clarify anything. Jytdog (talk) 15:18, 13 February 2018 (UTC)
- Here's my reply to Headbomb, posted over in that WT:MED discussion.
- [The proposed change, to add the word 'often'] is redundant and makes for clunkier wording. Ask around, you'll find that I'm as strong an advocate as any for recognizing the limits of WP:MEDDATE (and I get incredibly frustrated whenever someone slavishly and robotically declares a source "isn't MEDRS compliant!" solely because it's five years and one month old). Nevertheless, adding more and more qualifiers and caveats to the text of MEDRS isn't going to fix the problem. We already have:
- "This page...is a generally accepted standard that editors should attempt to follow, though it is best treated with common sense, and occasional exceptions may apply." (At the very top of the page)
- "Keeping an article up-to-date while maintaining the more-important goal of reliability is important." (Emphasis added)
- "These instructions...may need to be relaxed in areas where little progress is being made or where few reviews are published."
- "In many topics, a review that was conducted more than five or so years ago will have been superseded by more up-to-date ones, and editors should try to find those newer sources, to determine whether the expert opinion has changed since the older sources were written. The range of reviews you examine should be wide enough to catch at least one full review cycle, containing newer reviews written and published in the light of older ones and of more-recent primary studies."
- "While the most-recent reviews include later research results, this does not automatically give more weight to the most recent review..." (Emphasis added)
- "There are exceptions to these rules of thumb... A newer source which is of lower quality does not supersede an older source of higher quality."
- You're always going to have editors who want to interpret the guideline as a strict rule rather than a heuristic, no matter how much we water the wording down. Adding just one more caveat isn't going to magically turn on the lightbulb for an editor who isn't getting it. And if there is an article where the use of older reviews seems contentious, it's not necessarily a bad thing to have an actual discussion about it—not every problem is solved by smacking down your opponent with a WP:SHORTCUT link. TenOfAllTrades(talk) 15:24, 13 February 2018 (UTC)
Distinguishing "microbiology topics that may lead to medical applications" from "biomedical information"
Yesterday, news broke of the publication in Nature Microbiology of malacidin, a new class of antibiotic substance found from soil samples. The only experiments done to this point on it were to verify they could use genetic insertion to have a host body produce it in lab quantities, and did some preliminary tests for how well it could sterilize drug-resistant microbes in lab situations, including wound tests on rats. The researchers clearly are aware that if they can figure out how to produce this substance in larger batches, validate all the potential risk to health, it could be a possible antibiotic drug for humans, but that's years off.
However, some editors asserted that because it was being presented as an "antibiotic" (which generally implies "drug"), that the article's sourcing had to fall under MEDRS, and that with the Nature MB article being a primary source under MEDRS's definition, there were issues with sourcing and potential notability. This was related to posting this at WP:ITN/C where the general consensus there was that this was a microbiologic discovery, nothing yet to do with biomedical applications yet, and thus MEDRS did not apply. (See also Talk:Malacidin and Wikipedia talk:WikiProject Medicine).
I fully appreciate the need to keep new so-called "medical breakthroughs" (often junk science) to MEDRS standards, but I think there also needs to be a line where MEDRS does not cover microbiological research that is not yet ready for any type of human-based testing, and where sourcing is otherwise appropriate for a nominal science topic. Exactly where that is drawn I don't know if that is a bright line or a fuzzy one, but it should at least be when those researching such advances start making more specific claims about its effects on humans, rather than what they are seeing simple from standard microbiological testing on non-human subjects. To that, I think either MEDRS or the page Wikipedia:Biomedical information should reflect that basic, rather than applied, microbiological topics do not fall under MEDRS, and even applied microbiological topics should be evaluated if they are being presented as treating humans, or still in the early stages of refinement. An issue though is how that line should be drawn, and if it can be defined. --Masem (t) 16:44, 14 February 2018 (UTC)
- "including wound tests on rats" is very much going down the road of biomedical research. Nobody cares about curing rats of infections (and I know someone will bring up some ref about bubonic plague but that is not the point).
- I cannot tell you how often we deal with this kind of crap, from the scientists themselves, from overeager people who saw the news, from university PR people, etc. Please read WP:Why MEDRS?
- Here is my canonical example. You may or may not remember that scientist who published work showing that if you shake cells (really!) you could turn them into stem cells? There was huge media hype around that. And yep, people rushed to add content based on the hyped primary source to WP. (Note the edit date, and the date the paper came out) only to delete it later when the paper was retracted. (We actually have a whole article on that mess --Stimulus-triggered acquisition of pluripotency) We should not be jerking the public around like that. There is no reason to do that - we have no deadline here.
- Another example (I am copying this from "why MEDRS?") is news about health effects of food. Let's see, should I drink coffee or not? Maybe I will live longer and drive safer, and hey, if I am woman maybe I will be less depressed, but oh, no! it alters my estrogen levels and maybe it will screw up my baby. Every one of those links is from the New York Times (not some tabloid), and is just from the past few years. I think it is terrible to jerk the public around like this. A newspaper has an excuse, but Wikipedia does not — we need to provide reliable information to the public.
- The article about Malacidin is really too soon. It is frustrating that people gotta rush to add "hot news" but ... whatever. I should nominate that page for deletion but there are too many people who want to keep....
- Masem this is the same conversation we have been having at NOT. I am surprised to see you advocating for the "wikipedia is a newspaper" position here. Jytdog (talk) 17:55, 14 February 2018 (UTC)
- A lot of the content in Malacidin isn't about medical claims though, and it'd still be notable even if the antibiotic thing is found false; I wonder if attribution could help - rather than stating that it has x ability against pathogens etc, qualify the claim..
- I don't think not newspaper is relevant as it isn't routine coverage and it'll have notability + lasting coverage whatever happens to the claims about its abilities. Galobtter (pingó mió) 18:01, 14 February 2018 (UTC)
- (edit conflict)A couple points: first, taking the Stem Cell case, I see it was added only with primary sources. I would have to go back to look at any news coverage it got, but I completely agree that only primary sourcing here is bad; I would expect that to be properly included it should have had sources that included secondary commentary that agreed the science was sound. In the case of malacidin, we do have several news stories that include secondary commentary from microbiologists that agree this is a new class of antibiotics and the research is sound. It's not the same as corroborating articles, but there's enough there to justify why we are including that research at this stage.
- On the Not#news aspect, we are talking about a newly discovered class of antibiotics. On the presumption that that conclusion is true, that's clearly a fundamental topic in the field of antibiotics; we have a page for each class (see List of antibiotics), so having a page for this one is common sense. The only issue is the confirmation the class is legit from an independent lab, which likely will come in time. So here, while it is in the news, it is a topic that has permanence of importance as a fundamental scientific topic; creating and documenting at this time will only go to waste if the research is discovered to be flawed. Contrast that with the more common issue of Not#news coming up which is around he-said-she-said of politics and identity, where it is better to wait to avoid the controversy aspects than the objective facts. That's core here: we can document this in an objective manner, without worrying about any spin (outside of the hyperbole of the media for some aspects), NOT#NEWS is the problem when that can't be done. --Masem (t) 18:11, 14 February 2018 (UTC)
- Seeing how the Malicicin paper just published, the "lasting coverage" thing is out of place here, no? And experiments published exactly once, with no subsequent validation - is not an "objective fact". The paper published - that is a fact. But we don't know if the science in it is real yet, or if it will matter yet. Jytdog (talk) 18:13, 14 February 2018 (UTC)
- the claim that "permanence of importance as a fundamental scientific topic; " is unthinking bullshit - speech intended to persuade, without regard for truth. You can gussy it up all you want, but there is exactly one paper. It may be retracted next week. Again, see what I wrote about the "shaking cells" thing. Jytdog (talk) 18:15, 14 February 2018 (UTC)
- I'm not disagreeing that if this paper is called out as wrong (maybe these are already part of another class) then we should redact the article. But in contrast to the shaking cells, we have sources containing comments from other microbiologists who consider the work to be sound and valid. It's not 100% the work is truthful, but it seems to be on a lot better ground for being correct due to these other sources. Absolutely we need to eventually include those corroborating studies when they happen, but from how WP:N works here, there's plenty of reason to allow a standalone article (particularly since other classes of antibiotics have their own articles), as long as we consider that MEDRS should not yet apply to the microbiological aspects. --Masem (t) 18:23, 14 February 2018 (UTC)
- Which is why I was saying to attribute it instead of stating things as a fact. Galobtter (pingó mió) 18:28, 14 February 2018 (UTC)
- More yet on this. We have people looking to hype a company by trying to add primary source (scientific paper) by the company + press release from the company at Frequency Therapeutics
- We have people pounding at our articles at curcumin and other "natural products" trying to hype them based on primary sources and low quality reviews.
- we have really deadly shit about some quack doctor with a cure for sepsis (see here) that got news coverage and people went all gaga.
- This is all of a single piece. Early stage stuff being hyped. Whether it is PR people, or advocates for kooky stuff, or over eager people, it is all pushing preliminary work, taken out of the context of scientists talking to one another in the scientific literature, and trying to apply it, and using low quality refs to do it.
- Part of how MEDRS works is that we use it consistently, for all these kinds of things. Jytdog (talk) 18:10, 14 February 2018 (UTC)
- It may be "preliminary" as a medical topic, but from a microbiology standpoint, that presuming corroboration, a new class of antibiotics is fundamental. I used the analogy of a new chemical element here - same principle. If it turns out the antibiotic is lethal to humans, well, interest in it will wane, it won't gain any medical coverage, but it still remains a class of antibiotics; that cannot change (again, presuming corroboration). This is this part where MEDRS does not yet apply is covering it as a class of antibiotics (biology definition) rather than as a medical breakthrough, though we clearly should be informed by MEDRS not to drink the hype as a super-drug concept some news reports are pushing. (which I think the article clearly avoids, outside of establishing the problem this would help solve). --Masem (t) 18:15, 14 February 2018 (UTC)
- Please stop responding so quickly, and pause and think about what i am trying to communicate to you. You are writing unthinking bullshit. This one paper might be retracted next week or may not be replicable. You do not seem to understand how the scientific literature functions. Scientific papers are steps along the way to understanding. They are not Granite Fragments of Truth. They are "hey folks I did X and I think it means Y". It is where scientists talk to one another. Jytdog (talk) 18:17, 14 February 2018 (UTC)
- I've published, I know the process. What I'm saying for en.wiki is that in any other natural or physical science outside of medicine, that if a research paper published in a high-ranking journal like Science or Nature, introducing a new concept, and gets coverage by mainstream media in depth that establishes the importance of it, that material is usually included in WP with the research paper and the sources with secondary commentary - whether that be a new article or a section of one, doesn't matter for this purpose. No, there's no direct corroboration, but the topic presented by the paper is considered appropriate encyclopedic material to include with the ability to remove/redact should the paper be faulty. I fully appreciate that when we are talking anything that may be taken as potential medical advice that MEDRS needs to kick in and prevent that stuff until there is corroboration, working like BLP in that regard, but MEDRS wouldn't apply to most other physical and natural sciences, just as BLP doesn't apply to other topic areas. (This follows the same concept with announced published works, including those that end up being cancelled; we aren't a crystal ball, but a cancelled work that gained coverage prior to cancellation still remains a valid topic, and articles on such works as typically created when there is more than just announcement details that can be made). --Masem (t) 18:42, 14 February 2018 (UTC)
- Is it really true that people rush to add "hot science news" to WP in other fields? If so that is horrible. I did run across something like that... here at Plastic recycling. That was "hot news" about a "breakthrough" in a university lab. No sign that that this process is commercially feasible, or ever will be. (how could we know, right after the paper published)? But it was put in the section about how plastic is actually recycled (which is horrible by the way. Nobody reading that article will walk away understanding how plastic is actually recycled today -- what the actual industrial processes are.. which is a real failing on our part).
- That turned into a bigger issue with the user, DennisPietras, a retired scientist who mostly wanted to add "hot news" about science to WP and wrote here as a scientist, not as a WP editor. He ended up opening this discussion at the village pump about MEDRS, and filed an ANI against me, which went no where. Which is all too bad, because he could have been a great contributor, but never got aligned with the mission.
- We do have WP:SCIRS by the way. It too urges secondary sources, but gives more leeway for primary sources in other fields. I don't know how long it has been around, but it got elaborated some during some controversies when people were trying to make claims that some content was basic science, not medicine.....
- I should modulate here. Another reason why I won't nom the malacidin page for deletion is that it is ~likely~ that they will turn out to be at least a new class of "antibiotics" in the narrow sense of secondary metabolites bacteria use to compete with each other. I would never create this page at this time, but it is not worth the drama of going through deletion, and we can fix it up over time as we (humanity) actually win accepted knowledge about these molecules. But we (wikipedia editors) should include all the caveats by expert commentators about the preliminary nature of this as a class of 'antibiotics" in the common sense. Jytdog (talk) 19:06, 14 February 2018 (UTC)
- I wouldn't say every breakthrough is included, but I will stress that only those that come frmo high-ranking sources and get mainstream news coverage from quality RSes (BBC, NYTimes, etc.) are frequently included. An example is from this ITNC [[10]] (the #1.2 topic about the fossil). Including a scientific breakthrough only from the paper(s) primary to it should not happen, I fully agree, that's the case above you. We need secondary sources - even if we are talking mainstream - to establish importance and context as well as how to approach the topic is a less-technical manner. But we clearly don't push the MEDRS type levels of strict secondary sourced from peer-reviewed papers as the requirement elsewhere. And that's where this issue sits is that there's a point microbiology (a natural science) crosses into medicine, and we should be able to recognize when the topic is far less about medicine and more on the natural science. --Masem (t) 19:15, 14 February 2018 (UTC)
- ETA that reading SCIRS, we're still inline with that. It specifically allows news reports though appropriately cautions " Although news reports are inappropriate as reliable sources for the technical aspects of scientific results or theories, they may be useful when discussing non-technical context or impact of science topics, particularly controversial ones." Which we're not doing with the topic at hand. --Masem (t) 19:18, 14 February 2018 (UTC)
- I've published, I know the process. What I'm saying for en.wiki is that in any other natural or physical science outside of medicine, that if a research paper published in a high-ranking journal like Science or Nature, introducing a new concept, and gets coverage by mainstream media in depth that establishes the importance of it, that material is usually included in WP with the research paper and the sources with secondary commentary - whether that be a new article or a section of one, doesn't matter for this purpose. No, there's no direct corroboration, but the topic presented by the paper is considered appropriate encyclopedic material to include with the ability to remove/redact should the paper be faulty. I fully appreciate that when we are talking anything that may be taken as potential medical advice that MEDRS needs to kick in and prevent that stuff until there is corroboration, working like BLP in that regard, but MEDRS wouldn't apply to most other physical and natural sciences, just as BLP doesn't apply to other topic areas. (This follows the same concept with announced published works, including those that end up being cancelled; we aren't a crystal ball, but a cancelled work that gained coverage prior to cancellation still remains a valid topic, and articles on such works as typically created when there is more than just announcement details that can be made). --Masem (t) 18:42, 14 February 2018 (UTC)
- Please stop responding so quickly, and pause and think about what i am trying to communicate to you. You are writing unthinking bullshit. This one paper might be retracted next week or may not be replicable. You do not seem to understand how the scientific literature functions. Scientific papers are steps along the way to understanding. They are not Granite Fragments of Truth. They are "hey folks I did X and I think it means Y". It is where scientists talk to one another. Jytdog (talk) 18:17, 14 February 2018 (UTC)
- It may be "preliminary" as a medical topic, but from a microbiology standpoint, that presuming corroboration, a new class of antibiotics is fundamental. I used the analogy of a new chemical element here - same principle. If it turns out the antibiotic is lethal to humans, well, interest in it will wane, it won't gain any medical coverage, but it still remains a class of antibiotics; that cannot change (again, presuming corroboration). This is this part where MEDRS does not yet apply is covering it as a class of antibiotics (biology definition) rather than as a medical breakthrough, though we clearly should be informed by MEDRS not to drink the hype as a super-drug concept some news reports are pushing. (which I think the article clearly avoids, outside of establishing the problem this would help solve). --Masem (t) 18:15, 14 February 2018 (UTC)
- Depends greatly on the nature of the "breakthrough" and the amount and quality of the coverage it is getting in news sources. For example, first observation of gravitational waves was also just one paper at the time it was published (though it did have hundreds of authors). That work garnered mountains of media coverage, and had an 8000 word Wikipedia article within days. Subsequently, it is safe to say that the early impressions of its significance were absolutely correct, and the work has since led to a Nobel Prize. Of course, the discovery of malacidin is not remotely in the same category as the discovery of gravitational waves. Most research papers attract essentially no attention from the news media. Of those that do, only a few will attract broad or extensive coverage. Though such discoveries are a small minority, there is a reasonable case that those few scientific discoveries have enough general notability to be added to Wikipedia right away. If they are wrong, as happens sometimes, then the notability is often so well established already that we would still keep the article and provide corrected/updated information. Dragons flight (talk) 20:53, 14 February 2018 (UTC)
- Standing here now, and looking backward, and saying "see we were right about that!" is exactly the wrong thing to do. When science news breaks, we don't know at the time if it going to matter or not. Again, see the "shaking cells makes them into stem cells" thing. neither your nor anybody else has a crystal ball, science in the real world is nothing like in the movies, and in Wikipedia we do not give a flying fuck if the 24 hour news cycle latches onto some science paper that catches their fancy and hypes it. Jytdog (talk) 22:12, 14 February 2018 (UTC)
- Depends greatly on the nature of the "breakthrough" and the amount and quality of the coverage it is getting in news sources. For example, first observation of gravitational waves was also just one paper at the time it was published (though it did have hundreds of authors). That work garnered mountains of media coverage, and had an 8000 word Wikipedia article within days. Subsequently, it is safe to say that the early impressions of its significance were absolutely correct, and the work has since led to a Nobel Prize. Of course, the discovery of malacidin is not remotely in the same category as the discovery of gravitational waves. Most research papers attract essentially no attention from the news media. Of those that do, only a few will attract broad or extensive coverage. Though such discoveries are a small minority, there is a reasonable case that those few scientific discoveries have enough general notability to be added to Wikipedia right away. If they are wrong, as happens sometimes, then the notability is often so well established already that we would still keep the article and provide corrected/updated information. Dragons flight (talk) 20:53, 14 February 2018 (UTC)
- here is another really bad example. Virstatin. That page used to look like this. The first sentence of that used to be
References
- And the page was this whole elaborate bunch of nonsense. I came across this after I found this compound being discussed as an actual treatment for cholera elsewhere in WP. Turns out that this is a compound that was patented in 1986 (thirty years ago) and per our article, the activity against cholera was discovered in 2005. (13 years ago). I looked and found no sign of clinical development or any commercial or NGO involvement in making this an actual drug. So for now it is what we call a "tool compound" - something people use to do research.
- Bunch of hype based on primary microbiological research. Bad. Jytdog (talk) 18:36, 14 February 2018 (UTC)
- Based on this, the critical aspect of MEDRS applicability would seem to be when an article relates to a drug or purported drug. The article Virstatin in its current state seems to be OK. It's cholera protein inhibition is noted, but there's no claims that contravene MEDRS.
- What seems to be worth noting here is that an article on a bio-active compound has the clear potential for MEDRS-violating statements to be added to it (such as claims of viability as a drug), but this potential does not mean that the discussion of its bio-activity immediately needs to pass MEDRS standards for every statement. --LukeSurl t c 19:03, 14 February 2018 (UTC)
- User:LukeSurl you seem to have missed the purpose of virostatin example. yes it is fine now. :) Jytdog (talk) 20:14, 14 February 2018 (UTC)
- Yes it does. Once you start discussing bio-activity -
"these antibiotics only become active against bacteria in the presence of calcium" ... "Malacidins act by ... such interactions should not affect the cells of a host body and make the antibiotics non-toxic to the host"
etc. - you need secondary sources. Where's the proof that a compound becomes active against bacteria? Where's the proof that it should be non-toxic to the host? A primary source is not good enough for those claims. We know very well that experiments are subject to error and bias, which is why we insist on respecting secondary sources. We shouldn't have to be reminding editors of basic Wikipedia sourcing rules. --RexxS (talk) 19:25, 14 February 2018 (UTC)- The idea of "calcium-dependent antibiotic" is not new here - that's been established since at least... 1997? going by GScholar. How those function is known, the statements in there (sourced to news sources) are used to help the reader understand why this is important without being a microbiologist. The paper shows experiments that Malacidins follow the same behavior as previously identified calcium-dependent antibiotics. (The whole purpose of the research was to try to figure what DNA sequences helped a host to produce these Ca-dependent antibiotics) --Masem (t) 19:38, 14 February 2018 (UTC)
- Nobody's disputing that some chemicals have antibiotic action in the presence of calcium. I'd bet that we could find a secondary source to support that. What I want to know is what you're using to support your assertion that malacidins have antibiotic activity. So far I'm seeing a single report of some experiments (primary), and a handful of news outlets echoing that (just as primary). What are the good quality secondary sources, published in a respected journal that support your assertion? --RexxS (talk) 19:48, 14 February 2018 (UTC)
- If we go by SCIRS, we have secondary commentary from the news articles that include statements from uninvolved microbiologists that assert the validity of the work, though obviously not any immediately corroborating experiment. SCIRS doesn't require that. If we go by MEDRS, then we're lacking that. That's the problem here; if this was a core science topic nowhere close to MEDRS, there wouldn't be any issue. --Masem (t) 19:55, 14 February 2018 (UTC)
- see the plastic recyling thing above. Jytdog (talk) 22:13, 14 February 2018 (UTC)
- If we go by SCIRS, we have secondary commentary from the news articles that include statements from uninvolved microbiologists that assert the validity of the work, though obviously not any immediately corroborating experiment. SCIRS doesn't require that. If we go by MEDRS, then we're lacking that. That's the problem here; if this was a core science topic nowhere close to MEDRS, there wouldn't be any issue. --Masem (t) 19:55, 14 February 2018 (UTC)
- Nobody's disputing that some chemicals have antibiotic action in the presence of calcium. I'd bet that we could find a secondary source to support that. What I want to know is what you're using to support your assertion that malacidins have antibiotic activity. So far I'm seeing a single report of some experiments (primary), and a handful of news outlets echoing that (just as primary). What are the good quality secondary sources, published in a respected journal that support your assertion? --RexxS (talk) 19:48, 14 February 2018 (UTC)
- The idea of "calcium-dependent antibiotic" is not new here - that's been established since at least... 1997? going by GScholar. How those function is known, the statements in there (sourced to news sources) are used to help the reader understand why this is important without being a microbiologist. The paper shows experiments that Malacidins follow the same behavior as previously identified calcium-dependent antibiotics. (The whole purpose of the research was to try to figure what DNA sequences helped a host to produce these Ca-dependent antibiotics) --Masem (t) 19:38, 14 February 2018 (UTC)
- i have gone through the malacidin article, as have others, and have removed the medical-ish claims (e.g. it kills bacteria, it doesn't 'treat infections"). I also added that it will be years before we will know if this will be a drug, and that the scientists said that they are not trying to develop it. (A lot of the hoopla was about their method, and I wouldn't be surprised if they set up a company to discover more interesting chemicals using the method, but that is a different business.) I also replaced "antibiotic" in the first sentence with chemical made by bacteria - the underlying WL there is to secondary metabolite, which is definitely what this is from a microbiology standpoint. Jytdog (talk) 20:14, 14 February 2018 (UTC)
- I'll restress the one concern I mentioned, in that it seems like microbiologics would readily call this a "antibiotic", while biomed would reject that it is one. It's a problem of language choice here used by the RSes. I'm not thrilled that to move it out of MEDRS, remaining it to something not in the authoritative source is not helpful. Perhaps separately, we need "Antibiotic (microbiology)" and "Antibiotic (medicine)" articles to distinguish. --Masem (t) 01:16, 15 February 2018 (UTC)
- We strive to use plain english as much as possible per the WP:NOTJARGON policy. When there is possible confusion between the way a term is generally used and some technical use, of course we steer clear of the confusion. This is easily done by editing most of the time. calling this chemical an "antibiotic" in the lead and especially in an ITN blurb is just kind of blowing that off in favor of the hype. Jytdog (talk) 01:20, 15 February 2018 (UTC)
- Except that it is a antibiotic - to microbiologists. It seems wrong to shun one area of science by using a different term of art that has a different meaning in a different field. --Masem (t) 01:54, 15 February 2018 (UTC)
- Yes i acknowledged that. That isn't "except X" that is "I just ignored what you wrote". Say "antibiotic" and anybody with a high school education will think "drug to treat infections". (they won't even think "drug to treat bacterial infections". patients demanding doctors give them antibiotics for a cold or flu, and doctors giving them' remains a big problem. ) Sure the technical use can be used in the body, with some explanation. But it is not needed even there. microbiologists will understand plain english too. Jytdog (talk) 14:07, 15 February 2018 (UTC)
- But that begs that we should go through every article that is not using the "drug"-related version of "antibiotic" and switch the term out, ala Agar diffusion test (which is a microbiology article). Its a term of the art for MB's, not jargon. I fully support finding a way to make sure that when the word "antibiotic" is first used in an article that we establish it as the MB or biomedical version, even if we have to call the MB version a "microbiological antibiotic", so that the reader knows even if by the blue-link that it is not a drug. But to say we can't use this term at all because readers will take it to mean "drug" is not how we should be working. We recognize that context is fully important here, so articles are not required to meet the lowest-common denominator for language. --Masem (t) 14:46, 15 February 2018 (UTC)
- I think we should consistently clarify this, yes. I hope you aren't suggesting we use "microbiological antibiotic" as this is an eye-glazer (and even an antibiotic drug is a "microbiological antibiotic"). Maybe distinguishing by using "antibiotic drug" vs. "antibiotic chemical" or something? Whatever it is should work without the presence of the other term.... This specific issue arose due to the current ITN nomination and preventing the confusion that "there is a new antibiotic" from getting onto WP's front page. That should be our main concern for now.
- btw, even the Microbiology Society handles this gracelessly: under the big heading "WHAT ARE ANTIBIOTICS AND HOW DO THEY WORK?" they say: "Any substance that inhibits the growth and replication of a bacterium or kills it outright can be called an antibiotic. Antibiotics are a type of antimicrobial designed to target bacterial infections within (or on) the body."
 Facepalm Jytdog (talk) 15:37, 15 February 2018 (UTC)
Facepalm Jytdog (talk) 15:37, 15 February 2018 (UTC)
- Any type of differential we can make between the MB meaning and the BioMed meaning is going to clearly help to avoid MEDRS issues and the like.
- Incidentally, this NPR report suggests that the biology meaning was first, and usurped later in 1943 by the drug-related meaning. --Masem (t) 17:44, 15 February 2018 (UTC)
- the current lead of malacidins:
Malacidins are a class of chemicals made by bacteria found in soil that kill some Gram-positive bacteria. Their activity appears to be dependent on calcium. The discovery of malacidins was published in 2018. At the time of the publication it was not certain if the discovery would lead to any new antibiotic drugs; it takes years and millions of dollars to determine if a drug is safe and effective.
- at ITN, the alt 2 blurb:
The malacidins, a new class of antibacterial chemicals, are discovered.
- both of those are good enough for me. how about you? Jytdog (talk) 17:58, 15 February 2018 (UTC)
- I'm not sure. I'm concerned that we're basically washing away what the paper and those that were interviewed in news sources said "this is a new class of antibiotics" (using the MB definition). They're not just secondary metabolites, they're not just antibacterials either. It's a short-term solution that remains a long-term problem, and a mess on its own in the literature (when looking outside MEDRS sources). I don't know what else we can do beyond 1) making separate articles for the biological meaning and the medical meaning to help in blue-linking and hoverboxes, and 2) find a consistent way that we can name one or the other use (likely the microbiological use, given what you said on the more popular meaning of antibiotic) that keeps "antibiotic" but clarifies it as not a drug/medicine. But that's beyond the point of this discussion wrt to MEDRS. I think we've got it clear that just because there's a potential medical application, that as long as the science is not attempting to make any direct medical claims, MEDRS should not apply (SCIRS still does). --Masem (t) 18:07, 15 February 2018 (UTC)
- Where the literature is messy, WP will be as well.
- I think you meant to say "as long as the
sciencecontent is not attempting..." - With regard to that, it depends on how narrowly you are going to interpret "direct medical claims". As already noted, WP gets pounded on by advocates for all kinds things - people trying to hype or sell things based on "mouse studies" or the like. The reason they are doing that is the underlying human health issue. MEDRS will continue to apply in those kinds of situations. In my view the community is very (wonderfully and consistently) clear in its consensus on this kind of thing.
- the hype at the malacidin page has been dealt with enough, through editing, such that anyone reading it will know that the subject is basic science and that medicine is very, very far away. there is no health-driven hype in that page now. (it is still ridiculously sourced, but that is a function of TOOSOON and if this turns out to be real and is followed up on, we should be able to make it an actual WP article in a few years.)Jytdog (talk) 18:59, 15 February 2018 (UTC)
- (edit conflict) Of course MEDRS applies. The whole thrust of the Nature article is the potential for use of these chemicals in treating people. Of course commentators will speculate on the possibility in the popular press. That doesn't make a source meet what we ask for in MEDRS. It's just wikilawyering to try to hide that behind quibbles about "antibiotic" sometimes doesn't mean a drug used to treat bacterial infections in people. Every lay reader who sees a claim like "New class of antibiotic discovered" isn't going to think "oh that's interesting - a new chemical that some microbes use to kill other microbes"; they will be thinking "a new drug that can be used to treat infections that I might get". You can deny that all you want, but we all know it's true. And that is why such claims are subject to MEDRS, which applies to any biomedical claim in any article, even in articles that aren't regarded as primarily medical. --RexxS (talk) 19:01, 15 February 2018 (UTC)
- I'm not sure. I'm concerned that we're basically washing away what the paper and those that were interviewed in news sources said "this is a new class of antibiotics" (using the MB definition). They're not just secondary metabolites, they're not just antibacterials either. It's a short-term solution that remains a long-term problem, and a mess on its own in the literature (when looking outside MEDRS sources). I don't know what else we can do beyond 1) making separate articles for the biological meaning and the medical meaning to help in blue-linking and hoverboxes, and 2) find a consistent way that we can name one or the other use (likely the microbiological use, given what you said on the more popular meaning of antibiotic) that keeps "antibiotic" but clarifies it as not a drug/medicine. But that's beyond the point of this discussion wrt to MEDRS. I think we've got it clear that just because there's a potential medical application, that as long as the science is not attempting to make any direct medical claims, MEDRS should not apply (SCIRS still does). --Masem (t) 18:07, 15 February 2018 (UTC)
- the current lead of malacidins:
- But that begs that we should go through every article that is not using the "drug"-related version of "antibiotic" and switch the term out, ala Agar diffusion test (which is a microbiology article). Its a term of the art for MB's, not jargon. I fully support finding a way to make sure that when the word "antibiotic" is first used in an article that we establish it as the MB or biomedical version, even if we have to call the MB version a "microbiological antibiotic", so that the reader knows even if by the blue-link that it is not a drug. But to say we can't use this term at all because readers will take it to mean "drug" is not how we should be working. We recognize that context is fully important here, so articles are not required to meet the lowest-common denominator for language. --Masem (t) 14:46, 15 February 2018 (UTC)
- Yes i acknowledged that. That isn't "except X" that is "I just ignored what you wrote". Say "antibiotic" and anybody with a high school education will think "drug to treat infections". (they won't even think "drug to treat bacterial infections". patients demanding doctors give them antibiotics for a cold or flu, and doctors giving them' remains a big problem. ) Sure the technical use can be used in the body, with some explanation. But it is not needed even there. microbiologists will understand plain english too. Jytdog (talk) 14:07, 15 February 2018 (UTC)
- Except that it is a antibiotic - to microbiologists. It seems wrong to shun one area of science by using a different term of art that has a different meaning in a different field. --Masem (t) 01:54, 15 February 2018 (UTC)
- We strive to use plain english as much as possible per the WP:NOTJARGON policy. When there is possible confusion between the way a term is generally used and some technical use, of course we steer clear of the confusion. This is easily done by editing most of the time. calling this chemical an "antibiotic" in the lead and especially in an ITN blurb is just kind of blowing that off in favor of the hype. Jytdog (talk) 01:20, 15 February 2018 (UTC)
- I'll restress the one concern I mentioned, in that it seems like microbiologics would readily call this a "antibiotic", while biomed would reject that it is one. It's a problem of language choice here used by the RSes. I'm not thrilled that to move it out of MEDRS, remaining it to something not in the authoritative source is not helpful. Perhaps separately, we need "Antibiotic (microbiology)" and "Antibiotic (medicine)" articles to distinguish. --Masem (t) 01:16, 15 February 2018 (UTC)
- Thanks for talking Masem. As I said i believe the issues are resolved at the malacidins article and ITN through editing. See you around. Jytdog (talk) 19:15, 15 February 2018 (UTC)
Creep
This page has crept beyond WP:RS-- in order to stay in sync with the global guideline, it is intended to explain with respect to biomedical and health content how to apply RS. The writing could be tighter, and has some unnecessary redundancy, but there are also areas that deviate from WP:RS rather than interpret it or explain how to use RS with respect to medicine. As an example, see WP:BIASED, which is the en.Wikipedia-wide guideline on reliable sources, and compare what this page was saying. This page was saying, for example, that all editors had to agree to omit a source. This page is out of sync with WP:RS. There is a whole section on Conflict of interest, which we don't find at WP:V or WP:RS-- this page is intended to explain how to apply RS to medicine, and should not go beyond RS.
Tony1 is no longer editing for smoothing out the prose redundancies; perhaps @SlimVirgin: (who is probably one of Wikipedia's most experienced contributors to policy and guideline pages, and an excellent writer) can help restore this page to keep it aligned with WP:RS.
WP:BIASED (from WP:RS): |
WP:MEDBIAS (from WP:MEDRS): |
SandyGeorgia (Talk) 05:36, 3 April 2018 (UTC)
- @Francis Schonken:, I see you are the second editor after SarahSV at WP:RS.[11] This page has crept a lot over recent years; might you be interested in having a look? This is the page at the beginning of 2016. When the page was first started, there was intense focus on assuring it stayed within en.Wikipedia-wide guidelines so it could be elevated to a guideline.[12] SandyGeorgia (Talk) 05:51, 3 April 2018 (UTC)
- Tx for the ping. Re. WP:BIASED vs. WP:MEDBIAS: I couldn't tell whether in medical sources in general COI is a major topic w.r.t. bias. The recent Osmosis issue seems to confirm it might be the case however (and much of Carl Frederik's unrelenting litigation on the point seems to only further confirm it: "the
ladyWiki Project Med director doth protest too much, methinks"). If it is, then the current WP:MEDBIAS approach would be correct in pointing that out. In other areas (some of which are closer to my regular editing) COI would certainly not be a *major* bias-generating cause, so it is probably likewise defensible that the general RS guideline does not go in that amount of detail. - I'd suggest, instead of making general comparisons, you'd make rephrasing proposals, if you think that section (or any other) could be reworded to something more helpful in the context of medical articles.
- The whole guideline seems very elaborate, maybe too elaborate to be an effective tool. Anyway, if there are factual contradictions between the guidance given here, and the one contained in WP:RS, then the latter takes precedence I suppose, like WP:V takes precedence over WP:RS, etc. (compare WP:CONLEVEL). Some pruning might be quite in order, I suppose (compare Wikipedia:How to contribute to Wikipedia guidance#Pruning). Possibly. It's a bit out of my regular field of interest: I hope you guys can figure out what works best. Tx. --Francis Schonken (talk) 11:48, 3 April 2018 (UTC)
- Thanks, Francis. I wasn't viewing this in the context of the video situation, rather a need for some clarity in the overall writing, and to keep it in sync with project policy. (I already took a stab at it, but SV is a much better policy/guideline writer.) Less is more: I was also hoping for some writing help to get this page trimmed back to something more readable and manageable. I see wording that is going beyond the WP:V and WP:NPOV to give due weight to all majority and significant minority views. For example, the idea that all editors would agree to anything is amusing ;) Best, SandyGeorgia (Talk) 12:39, 3 April 2018 (UTC)
- It is a bit platitudes galore... personally I think "obvious or overt bias in a source is a difficult problem for Wikipedia" a much more disturbing platitude: "obvious or overt bias" is one of the easiest things to handle in Wikipedia (WP:NPOV), it's the covert variety that poses the real challenge. "If all editors on an article agree that a certain source should be omitted for this reason, it may rightfully be excluded" is of course a platitude too: sure, WP:CONSENSUS rules... if all editors on a medical article agree that a commercial flyer, promoting some brand of medication, is too "obvious"ly biased to consider it a reliable source, then of course consensus, and other guidance, dictates this source should be shown the exit. But I don't see how this is particularly helpful in the context of WP:MEDRS: as written it seems to steer for local consensuses trying to trump broader consensuses. And that's the real thing with platitudes: they're more often than not counterproductive, steering people in wrong directions and whatnot. --Francis Schonken (talk) 13:29, 3 April 2018 (UTC)
- Thanks, Francis. I wasn't viewing this in the context of the video situation, rather a need for some clarity in the overall writing, and to keep it in sync with project policy. (I already took a stab at it, but SV is a much better policy/guideline writer.) Less is more: I was also hoping for some writing help to get this page trimmed back to something more readable and manageable. I see wording that is going beyond the WP:V and WP:NPOV to give due weight to all majority and significant minority views. For example, the idea that all editors would agree to anything is amusing ;) Best, SandyGeorgia (Talk) 12:39, 3 April 2018 (UTC)
- Tx for the ping. Re. WP:BIASED vs. WP:MEDBIAS: I couldn't tell whether in medical sources in general COI is a major topic w.r.t. bias. The recent Osmosis issue seems to confirm it might be the case however (and much of Carl Frederik's unrelenting litigation on the point seems to only further confirm it: "the
- If you review the history of this talk page you will see that I and others like User:TenOfAllTrades have been trying to keep this simple and aligned with the other PAG, and an expression of community consensus that it (and other PAG) is and must remain. It could do with some trimming but the core is still solid. As written it does not try to steer people toward trumping community-wide consensus - it just emphasizes and explains what "secondary sources" are for content about health and why we rely on them.
- Given the context of the hopefully-starting-to-resolve video storm, which has already spilled into this discussion, I do not think that now is the best time to undertake a review of this very important guideline. Jytdog (talk) 13:45, 3 April 2018 (UTC)
- I agree that holding off is in order. Stated more explicitly: I agree that now is not the time to undertake this work, and hope we don't. I only had a look because I have been trying to sort out where this idea that leads have to be cited is coming from (per Doc James talk, but I just found it, at the Translation Project). In the meantime, we have to be aware that some (many?) editors are misapplying guidelines, and when we do have time to focus on it, the writing here really needs to be tightened. From the early days, when it took us TWO YEARS to get this page promoted to guideline, I have worried that it stay in sync so that it can continue to enjoy broad community support. SandyGeorgia (Talk) 14:03, 3 April 2018 (UTC)
How to identify reliable sources?
This guideline states "Ideal sources for biomedical information include: review articles (especially systematic reviews) published in reputable medical journals; ...".
Hence, many editors seem to favour publications from journals which are highly ranked, e.g. by impact factor (or a similar kind of metric) and tend to not accept publications from lower ranked journals. However, it's no clear whether highly ranked journals publish the more reliable results. In fact, recent data does not suggest that but rather the opposite (see the review Björn Brembs, Prestigious Science Journals Struggle to Reach Even Average Reliability, https://www.frontiersin.org/articles/10.3389/fnhum.2018.00037/full and references therein). To quote from the abstract of this review:
“However, data from several lines of evidence suggest that the methodological quality of scientific experiments does not increase with increasing rank of the journal. On the contrary, an accumulating body of evidence suggests the inverse: methodological quality and, consequently, reliability of published research works in several fields may be decreasing with increasing journal rank.“
Reliable and unreliable results can be found in higher and lower ranked journals. Decisions to use an article or not should be based on an evaluation of the content of the article not ‘its cover’. Lucleon (talk) 10:28, 8 March 2018 (UTC)
- Interesting, thanks. The guideline says "reputable" journals. There are plenty of lower ranked journals that are utterly reputable and MEDRS should support their use. In my own work in medical research, I cite the work I need to cite, I don't worry whether it's in, say, BMC Medical Informatics and Decision Making or Science. Both reputable, even if the latter has an impact factor many times larger than the former. Bondegezou (talk) 11:46, 8 March 2018 (UTC)
- Thanks for your reply, and I completely agree with you that also articles from lower rank journals can be cited in wikipedia (in research articles that is done anyhow). Only journals with an overall lack of quality in general (like predatory journals) should be categorically excluded. That was exactly my point.Lucleon (talk) 12:21, 8 March 2018 (UTC)
- But please read and understand WP:MEDRS and for making medical claims expect editors to be very insistant on high quality sources for making health related claims. If something you want to say can only be supported by something in a poorly ranked journal, expect scrutiny. As a newbie, the phrase that you highlighted above, "Ideal sources for biomedical information include: review articles (especially systematic reviews) published in reputable medical journals; ..." should be at the forefront of your mind. -Roxy, the dog. barcus 12:41, 8 March 2018 (UTC)
- If you use unambiguously high quality sources there will rarely be a problem. Please be aware that articles in Frontiers journals are often themselves poor quality or somebody running with their pet theories; many issues of Frontiers are "guest edited". Jytdog (talk) 13:11, 8 March 2018 (UTC)
- Thanks for your comments. Could you please give an example of an "unambiguously high quality source". Thank you.Lucleon (talk) 13:15, 8 March 2018 (UTC)
- May I also ask on which basis you claim that "articles in Frontiers journals are often themselves poor quality" and what the relevance of this statement for the cited Frontiers article is? For the cited article, the editor and the two reviewers are given on the Frontiers website. I would also be very interested if you have can refer to any data which is actually in contrast to the conclusions of the cited Frontiers article. Thank you. I appreciate your interest and input in this matter. Lucleon (talk) 13:24, 8 March 2018 (UTC)
- This is tedious and has nothing to do with building an encyclopedia. You need to decide if you are here to build an encyclopedia or WP:NOTHERE. I am uninterested in the kind of legalistic wrangling that you are demonstrating a tendency toward. If you aim high you will rarely go wrong and you and others will not have to waste time with this kind of unproductive discussion. Jytdog (talk) 13:47, 8 March 2018 (UTC)
- Discussing new data on the reliability of sources, seems crucial to me for an encyclopaedia. A discussion is unproductive if arguments are rejected by simply discrediting their source with no justification.Lucleon (talk) 13:58, 8 March 2018 (UTC)
- No. There is a lot of work to do. Are you here to build an encyclopedia or not? Based on your behavior, you are more interested in bickering. And we generally do not blow in the wind of the latest primary source - not with respect to content and not with respect to the policies and guidelines. Jytdog (talk) 14:02, 8 March 2018 (UTC)
- The article in Frontiers is a review article, not a primary source. Lucleon (talk) 14:08, 8 March 2018 (UTC)
- Yes it is, I was incorrect.
- Of your 34 edits to date exactly three have been to articles and the rest have been bickering. Please spend time actually building content, seeing what kinds of edits "stick" and which don't, doing your best to aim high per all the policies and guidelines and if you get reverted, please try to learn and aim higher the next time. Jytdog (talk) 14:13, 8 March 2018 (UTC)
- Starting an open discussion on recent investigations about the reliability of sources is bickering? Asking someone to explain unsubstantiated claims of the kind 'this journal is poor quality and therefore the article doesn't count' is bickering? Please explain me where you think I have been bickering in this thread. Lucleon (talk) 14:23, 8 March 2018 (UTC)
- See Sealioning. I am done here. Please work on building the encyclopedia. Jytdog (talk) 15:25, 8 March 2018 (UTC)
- Well, I didn't force you to take part in this discussion nor did I stalk you; so this has nothing to do with Sealioning. You make unsubstantiated claims and when kindly asked for clarification, you instantly question my motivation (please see WP:AGF), make ad-hominen arguments and - most importantly - still don't substantiate your arguments. That way a productive discussion is impossible. Please don't undermine the discussion of people who try to improve/maintain the quality of wikipedia. Lucleon (talk) 16:02, 8 March 2018 (UTC)
- See Sealioning. I am done here. Please work on building the encyclopedia. Jytdog (talk) 15:25, 8 March 2018 (UTC)
- Starting an open discussion on recent investigations about the reliability of sources is bickering? Asking someone to explain unsubstantiated claims of the kind 'this journal is poor quality and therefore the article doesn't count' is bickering? Please explain me where you think I have been bickering in this thread. Lucleon (talk) 14:23, 8 March 2018 (UTC)
- The article in Frontiers is a review article, not a primary source. Lucleon (talk) 14:08, 8 March 2018 (UTC)
- No. There is a lot of work to do. Are you here to build an encyclopedia or not? Based on your behavior, you are more interested in bickering. And we generally do not blow in the wind of the latest primary source - not with respect to content and not with respect to the policies and guidelines. Jytdog (talk) 14:02, 8 March 2018 (UTC)
- Discussing new data on the reliability of sources, seems crucial to me for an encyclopaedia. A discussion is unproductive if arguments are rejected by simply discrediting their source with no justification.Lucleon (talk) 13:58, 8 March 2018 (UTC)
- This is tedious and has nothing to do with building an encyclopedia. You need to decide if you are here to build an encyclopedia or WP:NOTHERE. I am uninterested in the kind of legalistic wrangling that you are demonstrating a tendency toward. If you aim high you will rarely go wrong and you and others will not have to waste time with this kind of unproductive discussion. Jytdog (talk) 13:47, 8 March 2018 (UTC)
- Thanks for your reply, and I completely agree with you that also articles from lower rank journals can be cited in wikipedia (in research articles that is done anyhow). Only journals with an overall lack of quality in general (like predatory journals) should be categorically excluded. That was exactly my point.Lucleon (talk) 12:21, 8 March 2018 (UTC)
Impact factor is still a useful metric. I read a study looking at this a while ago, and retractions are more common among low-impact factor journals. I didn't find the study in question right now, but the following support the statement:
- https://www.ncbi.nlm.nih.gov/pubmed/29516389
- http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1516-31802015005081601&lng=en&nrm=iso&tlng=en
- http://jme.bmj.com/content/37/2/113.long (states fraud is more common in high IF journals, but not retraction overall)
Will see if I can find the study I had in mind... Carl Fredrik talk 13:10, 9 March 2018 (UTC)
- Thanks for the feedback and the additional refs. The article I cited at the beginning of this section does actually discuss data from another study (https://www.ncbi.nlm.nih.gov/pubmed?Db=pubmed&Cmd=ShowDetailView&TermToSearch=21825063) that shows the opposite: retraction increases with impact factor. I would be very interested to see if there is maybe different data on the same issue and hence, it would be great if you could find the article that you are referring to. Thanks. Lucleon (talk) 16:34, 9 March 2018 (UTC)
Frontier journals have been labeled predatory per [[ https://predatoryjournals.com/publishers/ here] Doc James (talk · contribs · email) 21:02, 27 March 2018 (UTC)
- This list is essentially Beall's list - a list representing the opinion of a single individual, a list to which the addition of Frontiers has been very controversial (e.g. https://www.nature.com/news/backlash-after-frontiers-journals-added-to-list-of-questionable-publishers-1.18639; http://www.sciencemag.org/news/2017/01/mystery-controversial-list-predatory-publishers-disappears). Apart from that, the article cited above is from a highly reputable neuroscientist (Björn Brembs) and it's a review that summarises and discusses results from several other sources.Lucleon (talk) 22:15, 6 April 2018 (UTC)